Heart rate and cardiac conductivity disorders in junior athletes
ˑ:
Associate Professor, PhD V.V. Epishev1
Y.B. Korableva1
A.A. Bakushin1
Associate Professor O.B. Vedernikova1
1South Ural State University (National Research University), Chelyabinsk
Keywords: athletes, ECG, arrhythmia.
Introduction. Lack of rhythm in young athletes is usually due to the functional disturbances caused by various psychogenic, reflex and humoral disorders [2, 8]. Arrhythmia is a group of common cardiovascular diseases, characterized by the changes in the heart rate and cardiac conductivity [6]. Arrhythmias are divided into tachycardia, bradycardia, extrasystoles, and heart block, generally associated with the autonomic nervous system dysfunction [1]. Their early diagnosis and analysis can help prevent the development of pathological changes and protect the athlete’s health [3].
Objective of the study was to analyze the ECG variations in junior athletes competing in different sport disciplines.
Methods and structure of the study. Sampled and tested in 2015 through 2018 at the Scientific Research Center were the 16-18 year-old male athletes (n=302) representing different sports. The test data were mined by Bruce Treadmill Test using SCHILLER Cardiovit AT-104 test system, and processed by Statistica 10.0 software toolkit.
Results and discussion. Table 1 presents the data on the heart rate and cardiac conductivity disorders in the athletes.
Table 1. Heart rate and cardiac conductivity disorders in athletes competing in different sport disciplines (n=134)
|
Speed skating (n=10) |
||||
|
IRBBB |
Extrasystoles |
ERS |
Sinoatrial block |
Wandering pacemaker |
|
4 |
1 |
5 |
– |
– |
|
Track and field athletics (n=48) |
||||
|
16 |
7 |
19 |
5 |
1 |
|
Martial arts (n=22) |
||||
|
5 |
10 |
3 |
2 |
2 |
|
Cross-country skiing (n=24) |
||||
|
12 |
8 |
1 |
3 |
– |
|
Swimming (n=30) |
||||
|
16 |
10 |
– |
3 |
1 |
The table shows that IRBBB was detected in 53 athletes (39.55%) - representatives of 5 sports, thus indicating the predominance of the parasympathetic nervous system in these athletes. IRBBB was the most pronounced in the cross-country skiers and swimmers: 50.00 and 53.33%, respectively.
Extrasystoles were detected in 36 athletes (26.85%) - representatives of 5 sports - during the cycle ergometer test, possibly due to the increased tone of the sympathetic division of the autonomic nervous system. Extrasystoles were mostly typical of the combat athletes (45.45%).
ERS was diagnosed in 28 athletes (20.89%). As is known, ERS in athletes is usually a physiological effect of increased vagal tone. ERS was more pronounced in the representatives of speed skating (50.00%).
SA block was detected in 13 athletes (9.70%). It is the vegetative influences associated with the increased vagal tone that serve as a contributor to SA block, since the nucleus of the vagus nerve is the SA node. The highest frequency of SA block was observed in the cross-country skiers (12.50%).
Wandering pacemaker was registered in 4 athletes (2.99%), which was generally associated with the increased impact of the parasympathetic division of the autonomic nervous system on the heart or the sinus node malfunction. The heart automatism disorder - wandering pacemaker - was most significant (9.09%) in the group of combat athletes.
Below is the frequency of occurrence of the heart rate and cardiac conductivity disorders in different sports.
In speed skating (Fig. 1), IRBBB was observed in 4 athletes (40.00%), extrasystoles – in 1 (10.00%), ERS – in 5 (50.00%), while SA block and wandering pacemaker were not detected.
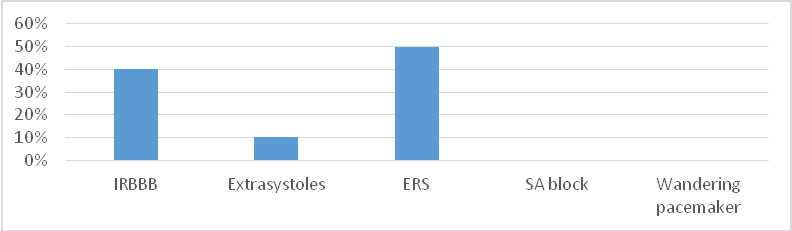
Fig. 1. Heart rate and cardiac conductivity disorders in speed skaters (%)
In track and field athletics (Fig. 2), IRBBB was observed in 16 athletes (33.33%), extrasystoles – in 7 (14.58%), ERS – in 19 (39.58%), SA block – in 5 (10, 41%), wandering pacemaker – in 1 (2.08%).
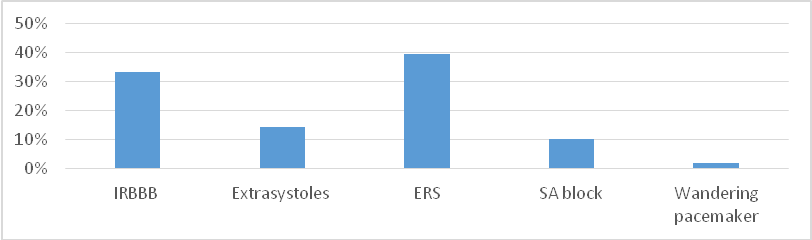
Fig. 2. Heart rate and cardiac conductivity disorders in track and field athletes (%)
Among the martial arts practitioners (Fig. 3), IRBBB was detected in 5 athletes (22.72%), extrasystoles – in 10 (45.45%), ERS – in 3 (13.63%), SA block - in 2 (9.09%), wandering pacemaker – in 2 (9.09%).
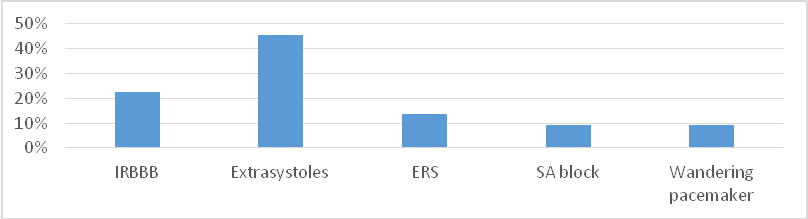
Fig. 3. Heart rate and cardiac conductivity disorders in combat athletes (%)
Among the cross-country skiers (Fig. 4), IRBBB was observed in 12 (50.00%), extrasystoles – in 8 (33.33%), ERS – in 1 (4.16%), SA block – in 3 (12.50%), while wandering pacemaker was not detected.
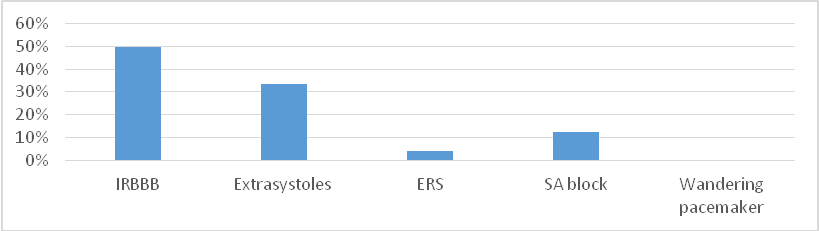
Fig. 4. Heart rate and cardiac conductivity disorders in cross-country skiers (%)
Among the swimmers (see Table), IRBBB was registered in 16 athletes (53.33%), extrasystoles – in 10 (33.33%), ERS – not detected, SA block – in 3 (10.00%), wandering pacemaker – in 1 (3.33%).
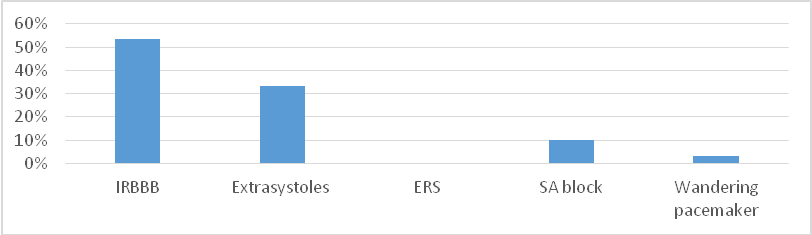
Fig. 5. Heart rate and cardiac conductivity disorders in swimmers (%)
Conclusion. The study data and analysis give us the grounds to conclude that the HR disorders are occasional i.e. non-associated with serious pathologies in anamnesis (manifested in short-term faints, syncope conditions, weakness, faintness etc.). It should be mentioned that the HR and cardiac conductivity disorders were not diagnosed in the intensive exercise tests. Therefore, the HR and cardiac conductivity disorders in the sample may be ranked with the functional versions of the sport form and, hence, shall not result in any limitations in the training process i.e. viewed as non-malignant developments showing no indications of regress towards unhealthy conditions.
The article was supported by the government of the Russian Federation (Act No. 211 of 03/16/2013), Contract No. 02.A03.21.0011. The study was performed as a part of the State Assignment of the Ministry of Education and Science of the Russian Federation (Grant No. 19.9733.2017/БЧ). The study was performed as a part of the State Assignment of the Ministry of Education and Science of the Russian Federation (Grant No. 19.9731.2017/БЧ).
References
- Chandra N. Sudden cardiac death in young athletes: Practical challenges and diagnostic dilemmas. Journal of the American College of Cardiology. 2013. No.61(10). pp. 1027-1040.
- Corrado D. Does sports activity enhance the risk of sudden death in adolescents and young adults? J. Am. Coll. Cardiol. 2003. No. 42(11). pp. 1959-1963.
- Delise P. Long-Term Effect of Continuing Sports Activity in Competitive Athletes With Frequent Ventricular Premature Complexes and Apparently Normal. Heart Am. J. Cardiol. 2013. No.112. pp. 1396-1402.
- Fuchs Т. The Clinical Significance of Ventricular Arrhythmias during an Exercise Test in Non-Competitive and Competitive Athletes. IMAJ. 2011. No.13. pp. 735-739.
- Drezner J.A. Electrocardiographic interpretation in athletes: the Seattle criteria. Br. J. Sports Med. 2013. no. 47. pp. 122-124.
- Kiss O. Prevalence of physiological and pathological electrocardiographic findings in Hungarian athletes. Acta Physiologica Hungarica. 2015. No.102(2). pp. 228-237.
- Verdile L. Exercise-induced ventricular tachyarrhythmia’s in athletes: do they have a different clinical significance? Math of Congress of Euro Prevent. Abstract book. 2013. No.33. pp. 176.
- Nikulina A.; Kozlov V.; Shukanov A. Changes in heart rate variability as a reflection of implemented physiological mechanisms of adaptation. HUMAN. SPORT. MEDICINE, [S.l.], v. 17, n. 4, p. 14-20, sep. 2018. doi: 10.14529/hsm170402
Corresponding author: epishevvv@susu.ru
Abstract
The study topic is in high priority at present due to the reported growth of the heart rate disorders in athletes and the still limited knowledge of the reasons for the HR disorders. Objective of the study was to analyze the ECG variations in junior athletes competing in different sport disciplines. Sampled and tested in 2015 through 2018 at the Scientific Research Center were the 16-18 year-old male athletes (n=302) representing different sports. The test data were mined by Bruce Treadmill Test using SCHILLER Cardiovit AT-104 test system, and processed by Statistica 10.0 software toolkit. The sample was diagnosed with the HR and cardiac conductivity disorders including incomplete right bundle-branch block (IRBBB) (39.55% of the sample); extrasystoles (26.85 %); early repolarization syndrome (ERS) (20.89%), sinoatrial (SA) block (9.69%); and wandering pacemaker (2,99 %). The study data and analysis give us the grounds to conclude that the HR disorders are occasional i.e. non-associated with serious pathologies in anamnesis (manifested in short-term faints, syncope conditions, weakness, faintness etc.). It should be mentioned that the HR and cardiac conductivity disorders were not diagnosed in the intensive exercise tests. Therefore, the HR and cardiac conductivity disorders in the sample may be ranked with the functional versions of the sport form and, hence, shall not result in any limitations in the training process i.e. viewed as non-malignant developments showing no indications of regress towards unhealthy conditions.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE