Therapeutic swimming model for treatment of postural disorders
Фотографии:

ˑ:
PhD, Associate Professor V.V. Drogomeretsky1
PhD, Associate Professor A.A. Tretyakov1
PhD, Associate Professor G.L. Nesterenko1
P.P. Kondratenko1
1Belgorod State National Research University, Belgorod
Keywords: students, scoliosis, board, physical education, postural disorders, treatment, therapeutic swimming.
Background. Efforts to treat early postural disorders in the academic educational period are often complicated by the little if any interest of students in the academic physical education services [6, 3, 4]. The disinterested students are reluctant in the practical training sessions, unprepared or unfit for elementary physical exercises, tend to dodge any physical tension and are generally undetermined in the academic physical education and sports (PES) process. Therefore, special initiatives need to be taken to physically activate this group, find and build up due motivations for the academic PES service on the whole; and develop and offer new physical training and health technologies to treat postural disorders [3, 4, 1].
The postural disorders correction initiatives require very specific and duly designed and managed health-improvement physical education tools customizable to the types and severity of the postural deformations. It should be confessed with regret that traditional health correction programs applied at national universities are too unspecific and, hence, inefficient for the specific postural disorders correction purposes. This situation urges the national research community take efforts to find new training models and tools for correction of postural disorders.
Objective of the study was to analyze practical benefits of the therapeutic swimming model for treatment of postural disorders applicable in the academic physical education curricula.
Methods and structure of the study. The therapeutic swimming model for correction of postural disorders was designed to include the following three modules.
Theoretical module offers a cycle of lectures to update the students on the structure of spinal column and musculoskeletal system, reasons for spinal disorders, pathological spinal curvatures and dysfunctions and associating health disorders, plus the modern corrective physical training and self-training tools applicable in the academic educational period.
Dynamic self-test module gives the means for the students to master basics of the self-testing techniques to diagnose postural disorders (by visual examinations; plumb-line tests; shoulder index calculation; and spine functionality tests) and associating health problems; and to keep track of the individual variations in the health condition in the corrective training process.
Practical training module offers sets of diagnosis-specific corrective education and training sessions, with every training stage (dynamic aerobic practices; isometric exercises; and relaxation cycles) designed to attain specific goals in the health correction process with the progress rating planar spinal curvature tests.
The first stage of the above practical training module (dynamic aerobic practices) is designed to improve the musculoskeletal system functionality and physically activate the trainees (for a physical inactivity is known to aggravate the spinal curvatures).
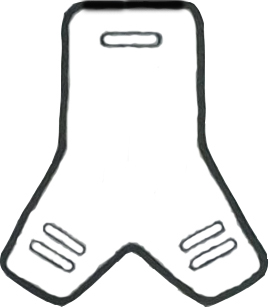
The second stage of the practical training module (static isometric exercises) is designed to improve functions of the major muscle groups to shape up a strong muscular corset, and develop the movement coordination and body balancing qualities with application of an experimental swimming board: see Figure 1 hereunder.
The third part of the practical training module (relaxation cycle) is designed to ease tension and relax every key muscle group plus shape up the imaginary ideal posture.
Each training session starts from the right posture shaping practices driven by the musculoskeletal sensations. The health correction practices are designed on a spine curvature specific basis. The associating health disorders in the sagittal-plane-curvature-diagnosed subgroup were found dominated (versus other subgroups) by body mass deficits; poor strength and coordination test indices; and poor static endurance of the major trunk muscle groups. The associating health disorders in the frontal-plane-curvature-diagnosed subgroup were dominated by the overall endurance deficits; and asymmetries of the static endurance test indices in the side trunk muscles. The primary diagnoses and tests were applied to customize the corrective practical training model to the postural disorders classified by the planar spinal curvatures.
Benefits of the new corrective practical training model were tested on Experimental Group (EG, n=20) and Reference Group (RG, n=20) of adolescent students, with every group composed of 2 planar-curvature-specific subgroups: see Table 1.
Table 1. EG and RG breakdown by the planar-curvature-specific subgroups
|
Spinal curvature plane |
EG |
RG |
|
Sagittal |
11 |
10 |
|
Frontal |
9 |
10 |
The EG was trained as required by the new corrective swimming model for one semester 2 times a week within the academic timeframe, plus once a week on a self-reliant basis on our instructions under control of the Physical Education Department in the S. Khorkina’s USK swimming pool of Belgorod Research University; and the RG was trained as required by the standard academic training curriculum.
The trainees’ progress in the new corrective swimming training process was rated by the following spinal curvature measurements: the frontal-curvature-diagnosed subgroups were tested by a photometric method to measure the spinal disorders by the summarized angles of asymmetry of the shoulder girdle, blades and posterior superior iliac spine; and the sagittal-curvature-diagnosed subgroups were tested by the brachial index calculations. The EG versus RG progress tests were run prior to and after the training sessions.
Study findings and discussion. Both EG subgroups were found to make progress in the postural disorder correction trainings. Thus the frontal-curvature-diagnosed EG subgroup showed significant reductions of the summarized angles of asymmetry upon completion of the corrective trainings (see Table 2) versus the RG trainees who made no progress in the spinal curvature test rates in the traditional academic physical education process.
Table 2. Postural correction progress rated by the summarized angles of asymmetry in the frontal-curvature-diagnosed EG subgroup versus the RG (α°)
|
Test time |
Summarized angles of asymmetry |
|
|
EG |
RG |
|
|
Pre-training tests |
29,3 ± 2,3 |
29,5 ± 2,2 |
|
Post-training tests |
13,4 ± 1,4* |
28,0 ± 2,3 |
Note: *statistically significant difference of the pre- versus post-training rates, p<0.05
The sagittal-curvature-diagnosed EG subgroup showed significant progress as verified by the growth of the brachial indices: see Table 3.
Table 3. Postural correction progress rated by the brachial indices in the sagittal-curvature-diagnosed EG subgroup versus the RG, %
|
Test time |
EG |
RG |
|
Pre-training tests |
73 ± 9,6 |
76 ± 9,4 |
|
Post-training tests |
95 ± 8,8* |
77 ± 8,4 |
Note: *statistically significant difference of the pre- versus post-training indices, p<0.05
It should be noted that in the primary tests the above indices were below 90% in the EG and RG that is indicative of the sagittal-plane spinal curvatures. Upon completion of the corrective trainings, the EG subgroup was tested with a significant growth of the shoulder indices to 95±8.8% versus the unvaried 77±8.4% in the RG.
The significant reductions of the summarized angles of asymmetry in the frontal-curvature-diagnosed EG subgroup and the significant growth of the brachial indices in the sagittal-curvature-diagnosed EG subgroup were interpreted as indicative of corrective effects of the new training practices.
The corrective tools applied by the new training model may be summarized as follows: moderate-intensity physical practices; special static and dynamic exercises combined with respiratory practices in different starting positions; special corrective exercises to reasonably combine muscular tension with relaxing and stretching elements; movement coordination and body balancing qualities building tools; special corrective exercises combined with dynamic and static short-time muscle tension; relaxing practices harmonized with breathing practices; asymmetric impacts on the musculoskeletal system; static postures etc.
Conclusion. The new corrective swimming model with application of the health physical training tools was designed to give a special priority to the due motivations for the physical progress and postural disorder treatment commitment building in the trainees in the diagnosis-specific physical trainings and muscular corset shaping practices.
References
- Bulgakova N.Zh. et al. Ozdorovitelnoe, lechebnoe i adaptivnoe plavanie. Ucheb. posobie dlya stud. vyssh. ucheb. zavedeniy [Health-improving, therapeutic and adaptive swimming. Study guide for students of higher ed. est.]. Moscow: Akademiya publ., 2005, 432 p.
- Drogomeretsk\y V.V., Tretyakov A.A., Agoshkov V.V. Poyas goniometricheskiy: pat. 174385 RF: MPK A 63 V 31/00 [Goniometer Belt: Pat. 174385 RF: IPC A 63 B 31/00]. Applicant and patentee BSNRU. no. 2017112366; appl. 11.04.2017; pupl.. 11.10.2017, Bul. no. 29
- Mirskaya N.B., Kolomenskaya A.N. Diagnostika narusheniy i zabolevaniy kostno-myishechnoy sistemy sovremennykh shkolnikov: podkhody, terminologiya, klassifikatsiya [Diagnostics of disorders and diseases of musculoskeletal system in modern schoolchildren: approaches, terminology, classification]. Vopr. sovremennoy pediatrii, 2009, vol. 8, no. 3, pp. 10-13.
- Moreva V.O. O narusheniyakh oporno-dvigatelnoy sistemy cheloveka [Musculoskeletal disorders in man]. Byul. meditsinskikh internet-konferentsiy, 2014, vol. 4, no. 5, P. 869.
- Onishchenko G.G., Baranov A.A., Kuchma V.R. Bezopasnoe buduschee detey Rossii: nauchno-metodicheskie osnovy podgotovki plana deystviy v oblasti okruzhayuschey sredy i zdorovya nashikh detey [Safe future of Russian children: scientific and methodological framework for preparation of action plan in the field of environment and health of Russian children]. Moscow: CHRC RAMS publ., 2004, 154 p.
-
Tretyakov A.A., Drogomeretsky V.V., Agoshkov V.V. Doska dlya zanyatiy plavaniem pri grudnom s-obraznom skolioze: pat. 166532 RF: MPK A 63 V 31/00 [Swimming board for training of patients with thoracic C-shaped scoliosis: Pat. 166532 RF: IPC A 63 B 31/00]. Applicant and patentee BSNRU». no. 2016109951/12; appl. 18.03.2016; publ. 27.11.2016, Bul. no. 33.
Corresponding author: pakhomova@bsu.edu.ru
Abstract
Mass postural disorders may be ranked among the most critical problems of the national youth population, with about 80% of the young people currently diagnosed with some postural disorders and/or spinal deformations. Postural disorders are known to be of detrimental effect to the functions of internal organs, cardiovascular, respiratory and digestive systems, plus on the physical and mental working capacity. The article analyzes practical benefits of the therapeutic swimming model for treatment of postural disorders. Subject to the study was Experimental and Reference Groups (EG, RG), with every group split up into 2 diagnosis-specific (planar spinal curvature) subgroups. The Experimental Group was trained for 1 semester 2 times a week (under the valid curriculum) as required by the health improvement model of our design; and the RG was trained under the traditional physical education curriculum – by the Physical Education Department in the S. Khorkina’s USK swimming pool of Belgorod Research University.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE