Oxygen supply for efficient muscular activity of middle-aged amateur mountaineers
Фотографии:

ˑ:
Dr.Hab., Associate Professor S.N. Litvinenko1
Dr.Biol., Associate Professor V.B. Voinov2
Dr.Biol., Professor E.V. Verbitsky2
PhD, Associate Professor Z.Kh. Sherkhov3
1Russian State University of Physical Education, Sport, Youth and Tourism (GTSOLIFK), Moscow
2Southern Scientific Center of Russian Academy of Sciences, Rostov-on-Don
3Kh.M. Berbekov Kabardino-Balkarian State University, Nalchik
Keywords: blood oxygenation, Holter ECG monitoring data, 4000-5400 m altitudes, cardiointervalograms, cardiac complex.
Introduction. Recently it has become a frequent practice for individuals without special mountaineering training to ascend to considerably high technically challenging altitudes. Such ascents of mountains are commercially-based and bear the form of tourism services that make climbing available for individuals of different ages and with different physical fitness levels. Nevertheless, mountaineers should exert great efforts, exceeding their everyday loads manifold, as well as overcome adverse environmental factors, primarily, hypoxia.
At the same time, the processes of high-altitude adaptation, characteristic of the given contingent, remain insufficiently studied. As a rule, the researchers focus their attention on elite athletes who regularly train at high or middle altitudes to improve their aerobic capacity [3, 4].
Objective of the research was to study the cardiorespiratory system performance rates in middle-aged people during high mountain expeditions at 4000-5400 m altitudes.
Methods and structure of the study. The study involved 6 people aged 30 to 62 years. Their oxygenation level (level of blood oxygen saturation in the finger tips) and pulse rate were measured in a relaxed sitting or prone position in a tent in the morning and in the evening using a portable pulse oximeter "AccuMed". The daily Holter ECG monitoring was carried out using the hardware-software complex "Valenta-MN-02-8.1" (LLC "Neo Company", St. Petersburg). The electrodes were placed in the tent at 7-8 p.m., then the subject fell asleep, woke up in the morning, performed his routine work, including high-altitude climbing, after which the ECG recording was stopped.
Results and discussion. The oxygenation and pulse rate values registered in the subjects are presented in Table 1.
Table 1. Oxygen supply rates at different altitudes
|
Indicator |
3400 m |
4350 m |
4900 m |
5400 m |
4350 m |
|
Pulse rate (bpm) |
78.8 ±10.9 |
84.2±9.6 |
80.6±8.1 |
79.8±6.5 |
80.3±6.1 |
|
Oxygenation (%) |
83.2±4.3 |
79.2±4.9 |
75.3±5.8 |
74.4±6.1 |
85.3±3.4 |
As Table 1 shows, the oxygenation level decreased as the subjects ascended to the altitude. However, having descended from 5400 m to 4350 m, they were found to experience the phenomenon of acclimatization: the degree of oxyhemoglobin in their blood increased significantly (p<0.05).
The study revealed that, during acclimatization, the aerobic indicators improved due to the reorganization in the cardiovascular system detected during the daily ECG monitoring.
It is known that the main acclimatization processes occur during night sleep at the altitude. Moreover, they can be either positively aimed to improve resistance to a set of high-altitude factors, primarily, hypoxia, or destructive, leading to serious disturbances in the body functions [1, 5].
In all the implementations of the sleep in the highlands we studied, we detected no regular alternation of the sleep phases, or smooth transition from phase to phase. At the same time, in a number of cases, we observed the ECG signs of the deep slow-wave sleep phase [1], which was realized by a single fragment, against the background of rapid transition - "falling out" of wakefulness or superficial sleep (Fig. 1). This indicates a significant need of the body for the anabolic processes of synthesis of the necessary hormones and metabolites, which occur specifically in the deep sleep phase.
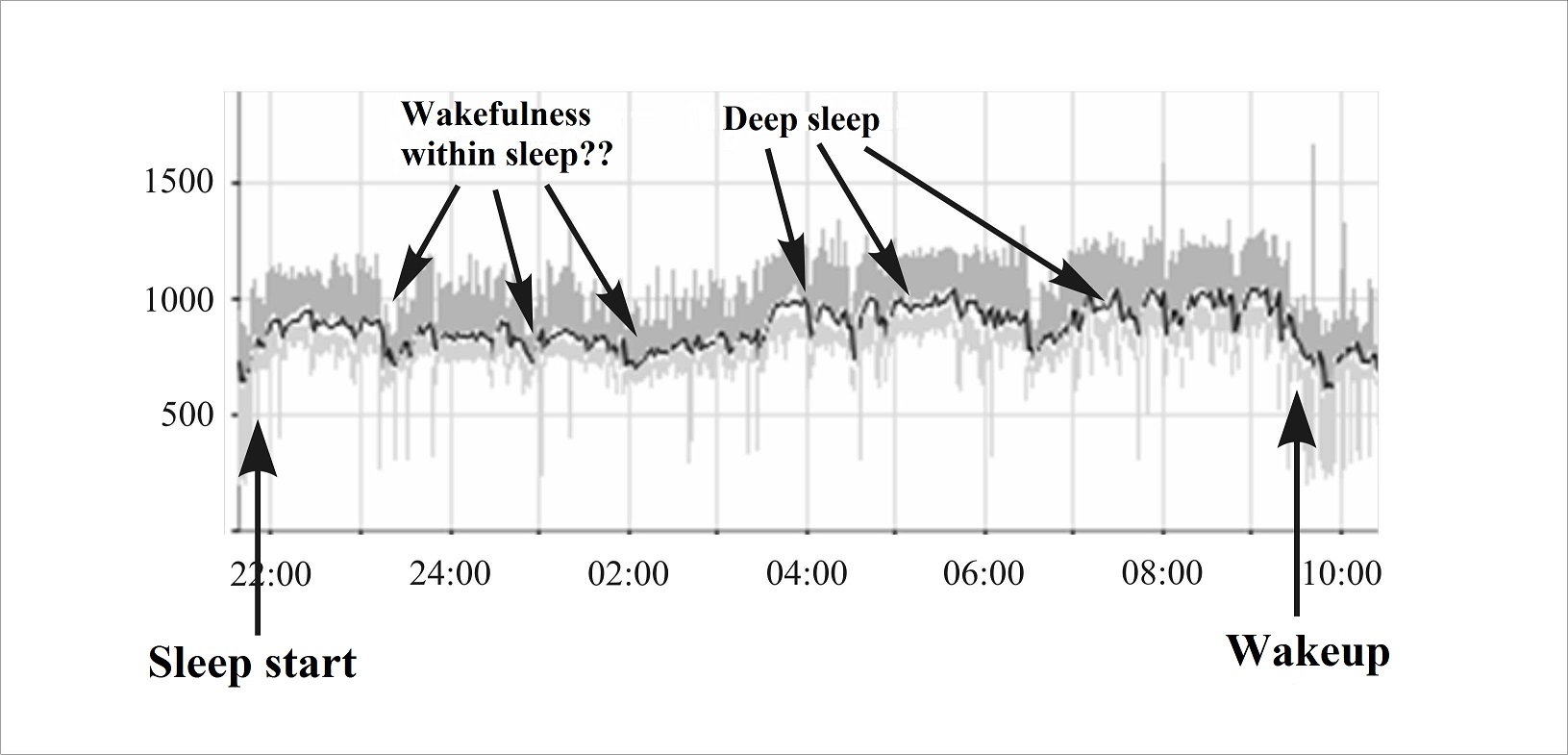
Fig. 1. Cardiointervalogram of Subject VVV (male, 62 y.o.). Altitude - 5380 m. X-axis - local time of examination, Y-axis - cardiointerval length in msec.
During the strenuous muscular activity, when ascending from the 4350 m to 5400 m altitude, the heart rate increased significantly (occasionally, up to 180-190 bpm) and the speed of movement decreased. At the beginning of the route, the step rhythm equaled 2.5 seconds per cycle; but further it increased to 6-7 seconds, including stops for up to 6 minutes (Fig. 2).
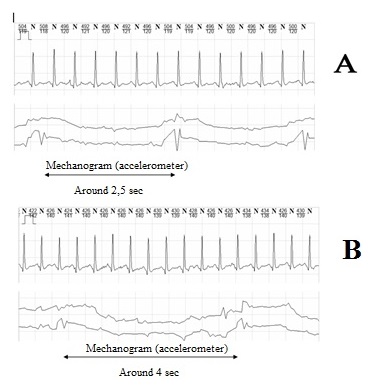
Fig. 2. ECG segments (lead CM5) and moto mechanograms at the beginning of the route (A) and after 5 hours of ascending (B). Subject - EN (male, 30 y.o.). Altitude A - 4350 m, altitude B - 5150 m.
When analyzing the parameters of variation pulsometry when ascending to the altitudes of 4800-5000 m, we detected a decrease in the overall heart rate variability, most pronounced in the high-frequency range of the cardiointervalogram spectrum (HF). In the background state, HF-component dominated in all subjects, amounting to 35-60% of the spectral power. Under maximum load, it decreased significantly. In addition, during the work, VLF component increased in all subjects, reaching 47-50%, having changed from the baseline by 20-30%. We assume that this may indicate the growing importance of anaerobic ergotropic mechanisms in terms of pronounced hypoxia (Fig. 3).
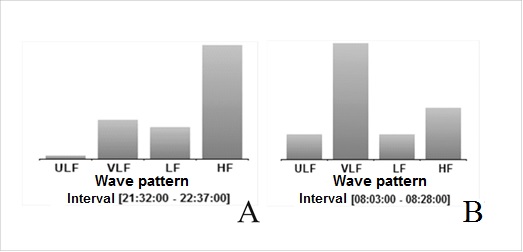
Fig. 3. Spectral characteristics of cardiointervalogram (A – sleep start, B - maximum strain during climbing).
When ascending to the altitude, significant changes were observed in the amplitude and length of various cardiac complex segments - significant depression of R wave, increase of S and T wave amplitude; ST-segment elevation, progressive decrease in the length of PQ, ST, RT intervals; certain narrowing of R wave (Fig. 4).
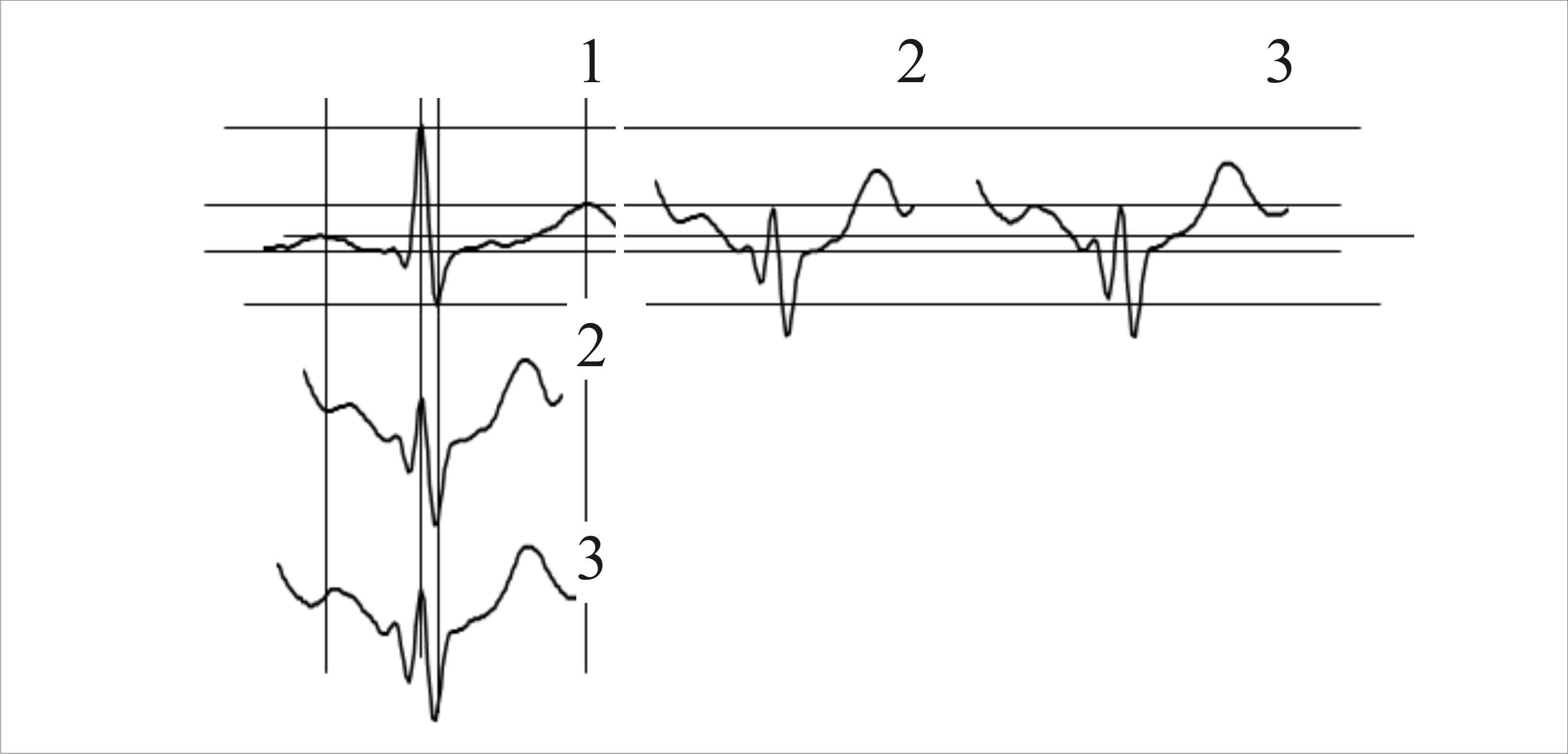
Fig. 4. Cardiac complex deformations during climbing. Subject - IL (male, 48 y.o.). 1 - quiet wakefulness (4050 m), 2 - beginning of the route (4350 m); 3 - continuation of the route (about 4700 m).
There have been recorded phenomena of ECG reorganization due to high-altitude hypoxia: shortening of R-R interval, increase of P wave, PQ elongation and flattening of T wave [6] or even its inversion [2]. In our opinion, certain differences in the observed phenomena can be explained by different altitudes at which the examination was carried out, as well as by different physical states of the subjects.
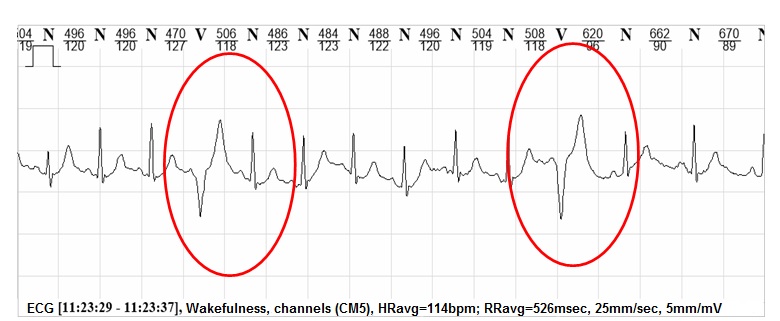
Fig. 5. Ventricular premature beats during mountain climbing. Subject - VVV (male, 62 y.o.). Altitude - 5380 m.
While walking at the altitudes of 5000 m or higher (HR of about 120 bpm), we registered numerous cases of ventricular premature beats not followed by a compensatory pause, which did not break the general contraction rhythm (Fig. 5), as well as single supraventricular premature beat, which testified to the signs of cardiac overstrain.
Conclusion. The participation of middle-aged people in high-altitude climbs without special training is accompanied by significant adaptive changes in the cardiorespiratory system resulting from high-altitude hypoxia combined with a continuous aerobic load, which jointly impose high demands on the oxygen supply in the body. At the altitudes below 5400 m the blood oxygen saturation considerably decreases and the cardiovascular system responds with tachycardia, changes in the spectral characteristics of the cardiointervalogram, heart rhythm disturbances, and cardiac complex deformation.
References
- Voinov V.B., Verbitskiy E.V. Issledovanie somnologicheskikh aspektov ostroy adaptatsii cheloveka k vysokogoryu [Study of the somnological aspects of acute adaptation of humans to the highlands]. Fiziologiya cheloveka, 2014, vol. 40, no. 6, pp. 46–57.
- Ryabtsev S.M. Kholterovskoe monitorirovanie EKG u alpinistov pri vysokogornykh voskhozhdeniyakh [Holter monitoring for climbers' ECG in high-altitude climbs]. Sovremennye problemy nauki i obrazovaniya, 2007, no. 1, pp. 130-131
- Suslov F.P., Hippenreiter J.B., Kholodov J.K. Sportivnaya trenirovka v usloviyakh srednegorya [Sports training in middle altitude conditions]. Moscow: RSAPC publ., 1999, 202 p.
- Timushkin A.V. Proektirovanie trenirovki kvalifitsirovannykh sportsmenov v usloviyakh vysokogorya. Avtoref. dis. dokt. ped. nauk [Training process design for skilled athletes in the highlands. Doct. Diss. abstract]. Balashov publ., 1998, 48 p.
- Chin K., Ohi M., Hirai M. et al. Breathing during sleep with mild hypoxia. Journal of Applied Physiology, 1989, vol. 67, no. 3, pp.1198-1207.
- Koller E. A., Drechsel S., Hess T., Macherel P., Boutellier U. Effects of atropine and propranolol on the respiratory, circulatory, and ECG responses to high altitude in man. European Journal of Applied Physiology and Occupational Physiology, 1988, no. 57, pp. 163-172.
Corresponding author: litvinenko_svetlana@yahoo.com
Abstract
The study was designed to obtain the blood oxygenation rates plus daily Holter ECG monitoring data in the mountaineering process, with 6 amateur mountaineers of 30 to 62 years of age having no special mountaineering background being subject to the study. The combined effect of the high altitude hypoxia and long aerobic muscular loads were found to significantly suppress the blood saturation with haemoglobin (under 74% on average) at up to 5400 m altitudes. A variety of disorders in the cardiovascular system performance were traced in the bodily hypoxic adaptation process including tachycardia, extra-systole and cardiac complex deformations.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE