Effects of hypoventilation breathing on physical working capacity during exercise to failure
Фотографии:

ˑ:
Professor, member-correspondent of Russian Academy of Medical Sciences N.A. Fudin1
PhD S.Y. Klassina1
Professor, Dr.Med. Y.E. Vagin2
1Research Institute of Normal Physiology named after P.K. Anokhin, Russian Academy of Medical Sciences, Moscow
2First Moscow State Medical University named after I.M. Sechenov, Ministry of Health and Social Development of the Russian Federation, Moscow
Keywords: sports, failure to exercise, voluntary hypoventilation, physical working capacity.
Introduction. Hypoventilation breathing is one of the most effective non-drug methods used to affect an external link of self-regulation of breathing and the functional status of the human body. This method is accompanied by changes in gas homeostasis and formation of a new economic breathing pattern against the background of the voluntarily programmed respiratory activity of man. It was found that long-term breathing training with altered respiratory volume (RV) and respiratory rate (RR) can result in the development of a new dynamic breathing pattern that would change gas composition of alveolar air and arterial blood [4-6].
The research objective was to study the effects of hypoventilation breathing on physical working capacity of individuals during exercise to failure.
Methods and structure of the study. Subject to survey were 13 apparently healthy young males of 18-22 years of age doing physical culture and sports on a regular basis. Each testee was subject to two identical surveys, during which he was asked to perform physical work to failure on a cycle ergometer at the constant cadence of 1 rps. In between the 1st and the 2nd tests, the subjects have been learning hypoventilation breathing (HVB) technique for 30 days. HVB technique teaching process was based on the respiratory training focused on the formation in the testees of the slow breathing pattern according to the system as follows: short inhale and exhale, but with a long, 10-15 sec, pause. Training was carried out on verbal instruction 3 times a week 1.5-2 hours each.
During the study, the subjects were in the following functional statuses: "background" (2.5 min), when blood pressure (BP), external respiration indices and timed inspiratory capacity (sec) were measured while the subjects were sitting on a cycle ergometer; "warm up: 60 W" (2 min); "exercise stress test to failure" at the load power of 120 Watts. The load testing duration was determined by the failure of the subject to perform exercise further (T-failure, sec). After exercise, BP, external respiration indices and timed inspiratory capacity (sec) rates were measured once again.
Exercise stress test was conducted using the cycle ergometer "Sports Art 5005". The ECG and pneumogram-guided test was carried out by means of the digital ECG system Poly-Spectrum-8 (Neurosoft, Russia). The following physiological parameters were estimated: heart rate (HR, bpm) and respiratory rate (RR, 1/min), ECG waves and segments [7, 8].
In the background and after exercise we measured timed inspiratory capacity (t/i, sec), systolic (SBP, mmHg) and diastolic (DBP, mmHg) blood pressure, external respiration indices: vital capacity (VC, l), forced vital capacity (FVC, l), forced expiratory volume in the 1st sec (FEV1, l). The indices were registered using the SP-1 portable spirometer. By means of calculation we assessed stroke volume (SV, ml) and minute volume of the heart (MVH, l/min), Kerdo vegetative index (KVI, %) [1].
Total EMG of the quadriceps muscle of the right thigh was recorded by means of the computer electromyography system Neurotech (Taganrog, Russia). We analyzed the average EMG amplitude (mV) and the number of turns, as they show the strength of muscle contraction and alpha motor neuron impulsation rate in the active phases of movement [2]. EMG was registered during warm-up and exercising in the last 30 sec.
The statistical processing of the experimental material was made using the mathematical methods of statistics. The significance of differences of the indicators was estimated using the non-parametric Wilcoxon test.
Results and discussion. Of all the vegetative functions breathing is the only one that can be voluntarily influenced by an individual, which thereby may change the operating mode of other physiological functions. The effectiveness of formation of HVB in the subjects can be estimated by the dynamics of the timed inspiratory capacity indices in the background before and after the HVB training. The analysis of the timed inspiratory capacity indices before and after the HVB training revealed that the HVB technique mastering program was successful, as breath hold duration increased (see Table 1). This fact suggests that the subjects’ ventilation hypoxia tolerance has improved after the HVB training.
The HVB technique mastering process influenced the subjects’ functional status, as reflected in the changes of the baseline vegetative indices obtained during the 2nd test (see Table 1).
Table 1. Baseline vegetative indices during 1st and 2nd tests, M±m
|
Indicators |
Background-1 |
Background-2 |
|
SBP, mm Hg |
125.0 ±3.3 |
119.5±4.0 |
|
DBP, mm Hg |
69.3±2.3 |
70.5±2.5 |
|
SV, ml |
74.7±2.3 |
82.1±2.8 p<0.05 |
|
MVH, l/min |
6.3±0.3 |
7.1±0.3 p<0.05 |
|
HR, bpm |
84.5±2.8 |
86.9±3.3 |
|
KVI, % |
16.7±4.2 |
17.8±3.6 |
|
VC, l |
4.0±0.3 |
4.1±0.2 |
|
IТ, % |
83.8±3.8 |
87.8±1.6 |
|
RV, l |
0.5±0.03 |
0.5±0.02 |
|
RR, 1/min |
18.6±1.3 |
17.5±1.2 |
|
RMV, l/min |
9.1±0.8 |
8.4±0.6 |
|
T/i, sec |
64.5±12.4 |
112.2±15.2 p<0.05 |
As Table shows, after the HVB training the subjects tended to have increased HR and KVI, which testifies to the strengthening of the sympathetic effects on the heart. Against the background of practically stable blood pressure, the testees were observed to have a significant increase of SV and MBV, which suggests an enhancement of tissue oxygen utilization and, thus, the level of physical working capacity [4]. Under the influence of HVB, the HR and RMV indices tended to decrease, which can be regarded as a tendency towards "economization" of breathing [3]. Consequently, the formed HVB promoted increased sympathetic effects on the heart of the subjects, intensification of the circulatory function, respiratory rate reduction in terms of constant respiratory volume.
Developing fatigue is a combination of changes occurring in various organs, systems and body in general during physical work and, as a result, making its further performance impossible, i.e. causing exercise task failure. The analysis of the EMG parameters showed that during the 1st survey the average EMG amplitude at task failure amounted to 1.7±0.3 mV, and during the 2nd survey (against the background of HVB) was lower and amounted to 1.4±0.1 mV. The number of turns at task failure equaled 3293±518 in the 1st test, which was significantly higher than during warming up - 2060±209 (p<0.05). This is indicative of a large number of alpha motor neurons activated at task failure. In the 2nd test (against the background of HVB) there was a less pronounced increase in the number of turns, which amounted to 2072±175 and 2321±139 during warming up and exercising, respectively. We believe that the downward trend in muscle force and a significant reduction of the firing rate of alpha motoneurons at task failure against the background of HVB is determined by the changes in the state of cortical nerve centers due to the developed fatigue.
Fatigue may result from the changes in the activity of the vegetative support systems, primarily the respiratory and cardiovascular ones. However, the most important consequence of such changes is reduced oxygen transport capacity of the body [3]. Thus, before the HVB training program applied performance of exercise to failure in comparison with the background values (Table 1) caused an increase of HR – up to 99.1±3.7 bpm (p<0.05) and of RR – up to 19.5±1.4 1/min, but it slightly changed the background values of MVH and MVR, which amounted to 6.3±0.6 and 9.0±0.8, respectively. After the HBV training, performance of the same exercise to failure as compared to the background values (see Table 2) resulted in the increase of HR up to 101.0±5.5 bpm (p<0.05) and an upward trend in MBV- up to 7.85±0.5 l/min, as well as a significant reduction of RR - to 10.3±0.9 1/min (p<0.05) and MRV - up to 5.3±0.6 l/min (p<0.05).
All this suggests that, against the background of hypoventilation breathing, performance of the same exercise to failure did not promote a reduction of the oxygen transport capacities of the body but, on the contrary, enhanced them. This can be seen in the tendency for increase of MVH and significant decrease of HR and MRV, i.e. in the improvement of the oxygen uptake in tissues [1] and economization of breathing [3].
It is known that the subject's task failure is accompanied by severe hypoxia [8]. As follows from the analysis of the ECG waves and segments, while Q wave depth at task failure was equal to -0.3±0.04 mV during the 1st examination, during the 2nd one (against the background of HVB) Q wave was not that deep and equaled -0.2±0.05 mV, which can be considered as a reduction of myocardial oxygen supply deficit. Thus, HVB applied during exercise to failure promotes myocardial oxygen supply.
Figure 1 illustrates the histograms of the mean time of training to failure before and after the HVB training.
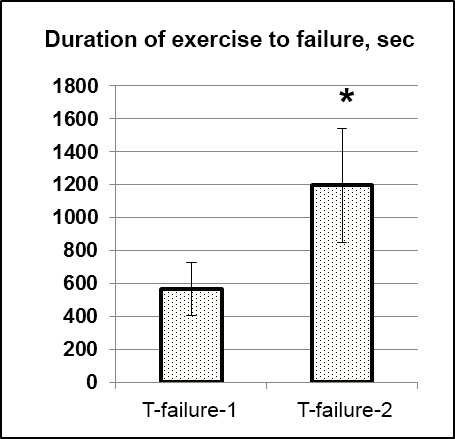
Figure 1. Mean time of training to failure before (T-failure-1) and after (T-failure-2) HVB training
As seen from Figure 1, HVB stipulated a twofold increase in the duration of exercise to failure (p<0.05), i.e. a twofold increase of physical working capacity of the testees.
Conclusion. Against the background of voluntarily formed hypoventilation breathing, there was registered an enhancement of ventilation and motor hypoxia tolerance, increase in the sympathetic effects, SV and MVH indices, improvement of oxygen uptake in tissues against the background of economic breathing. Moreover, myocardial oxygen supply was improved too, which in the end resulted in a twofold increase of physical working capacity.
References
- Karpman V.L. Dinamika krovoobrashcheniya u sportsmenov (Circulatory dynamics in athletes) / V.L. Karpman, B.G. Lyubina. – Moscow, 1982. – 135 p.
- Komantsev V.N. Metodicheskie osnovy klinicheskoy elektroneyromiografii (Methodical basics of clinical electroneuromyography) / V.N. Komantsev. – St. Petersburg, 2001. – 350 p.
- Kotz Y.M. Sportivnaya fiziologiya (Sport Physiology): textbook for physical culture institutes / Y.M. Kotz. – Moscow: Fizkultura i sport, 1998. – 200 p.
- 4Fudin N.A. Fiziologicheskaya tselesoobraznost' proizvol'noy regulyatsii dykhaniya u sportsmenov (Physiological feasibility of voluntary regulation of breathing in athletes) // Teoriya i praktika fiz. kultury. – 1983. – № 2. – P. 21-22.
- Fudin N.A. Gazovy gomeostazis (proizvol'noe formirovanie novogo stereotipa dykhaniya) (Gas homeostasis (arbitrary formation of new breathing stereotype) / Gen. ed. K.V. Sudakov. – Tula: Tulskiy poligrafist, 2004. – 216 p.
- Fudin N.A., Khadartsev A.A., Orlov V.A. Mediko-biologicheskie tekhnologii v sporte (Medicobiological technologies in sport) / Ed. by RAS and RAMS acad. S.P. Smirnov. – Moscow, 2011. – 460 p.
- Fudin N.A. Vzaimosvyaz' pokazateley myshechnoy i serdechno-sosudistoy sistem pri vozrastayuchshey fizicheskoy nagruzke u lits, zanimayushchikhsya fizicheskoy kul'turoy i sportom (Correlation of muscular and cardiovascular system characteristics at step load in persons engaged in physical culture and sport) / N.A. Fudin, S.Y. Klassina, S.N. Pigareva // Fiziologiya cheloveka (Human Physiology). – 2015. – V. 41 – № 4. – P. 82-90.
- Fudin N.A., Klassina S.Y., Pigareva S.N., Vagin Y.E. Analiz pokazateley elektrokardiogrammy i elektromiogrammy v moment prekrashcheniya vypolneniya intensivnoy fizicheskoy raboty u lits, zanimayushchikhsya fizicheskoy kul'turoy (Analysis of electrocardiogram and electromyogram indices at task failure in persons doing sports) // Sportivnaya meditsina: nauka i praktika. – 2015. – № 3. – P. 31-37.
Corresponding author: klassina@mail.ru
Abstract
Research objective was to study the effects of hypoventilation breathing on physical working capacity of individuals during exercise to failure on a cycle ergometer. Subject to survey were 13 apparently healthy young males of 18-22 years of age doing physical culture and sports on a regular basis. Each subject was surveyed twice, during the surveys he was asked to perform exercise to failure on a cycle ergometer at the constant cadence of 1 rps. In between the 1st and the 2nd tests, the subjects have been learning hypoventilation breathing (HVB) technique for 30 days. It is shown that, against the background of HVB, there is an enhancement of ventilation and motor hypoxia tolerance. At the same time, there occurs an increase in the sympathetic effects, minute volume of the heart, tissue oxygen utilization, "economization" of respiration, which in the end leads to a significant improvement of physical working capacity.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE