Muscle and cardiovascular indicators in persons engaged in physical culture and sport at the time of failure to perform strenuous physical exercise
Фотографии:

ˑ:
Corresponding member of RAS, Professor N.A. Fudin1
Ph.D. S.Yu. Klassina1
Ph.D. S.N. Pigareva1
Professor Yu.E. Vagin2
1P.K. Anokhin Research Institute of Normal Physiology, Moscow
2I.M. Sechenov First Moscow State Medical University, Moscow
Keywords: sport, endurance exercise, exercise to failure, endurance.
Introduction. Strenuous physical exercises contribute to physical improvement of an athlete only when the load is optimal for his/her body. Excessive (or endurance) exercise is adverse for athletes since it can cause failure of adaptation.
The research objective was to study hemodynamic characteristics and ECG and EMG indices of athletes at the time of failure to perform strenuous exercise.
Research methods and organisation. Subject to study were 25 males aged 18-19 years engaged in physical culture and sports. Step load to failure on a cycle ergometer was offered to each of them. The subjects went through the following stages of the load: “background” (2.5 minutes); “warm-up 60 W” (2 minutes); “step load with a step of 20 W, from 60 W to 120 W” against the background of the constant pedaling speed of 7 km/hour (1 minute for each load stage); physical load to muscular failure at the stage of 140 W against the background of the constant pedaling speed 7 km/hour; “recovery” (6 minutes).
Cycle ergometer “Sport Art 5005” was used for load testing, while the testing itself was conducted under control of ECG and EMG. Total EMG of the quadriceps muscle of the right thigh was recorded, followed by an analysis of the mean amplitude (Aavg, mV) and the number of turns [1, 3]. ECG was recorded in the I standard lead and "V5" lead. Heart rate (HR, beats/minute), waves and segments of ECG were assessed. Kerdo index (KI, %), stroke volume (SV, ml) and minute blood volume (MBV, l/min) were calculated [2].
“SIGMA-bc-509” device (Germany) was used to register pedaling speed. Blood pressure was measured in the background, at the time of muscular failure and 6 minutes after recovery. The subjective health status was rated on a five-point scale.
Statistical processing of the obtained data was performed using nonparametric criteria.
Research results and discussion. At the time of muscular failure the bodies of the subjects were close to the “limit” of their physiological capabilities, and it allows us to regard their functional state as marginal, reflected in the values of the indicators of physiological functions. Significant strengthening of sympathetic effects on the heart was noted, with the increase of Kerdo index from 13.1 ± 2.6 to 58.4 ± 2.4% (p<0.05), increase of systolic blood pressure from 122.6 ± 2.2 to 150.7 ± 3.9 mm Hg (p<0.05) and a upward trend of diastolic blood pressure testifying in its favor. Stroke volume increased significantly – from 69.7 ± 2.1 to 82.2 ± 5.1 ml (p<0.05) as well as minute blood volume – from 5.9 ± 0.2 to 14.8 ± 1.1 l/min (p<0.05). It is known that in case of physical performance the minute blood volume reflects the intensity of oxygen consumption by the tissues, and its maximum is an indication of the functional reserve of the cardiorespiratory system of an athlete [2]. This implies that strenuous exercise to failure led to a more than twofold increase of the minute blood volume – 14.8 ± 1.1 l/min, which determines the marginal capabilities of the subjects. It should be noted that after the recovery Kerdo index and hemodynamic indicators returned to baseline values.
Analysis of ECG waves and segments revealed that at the time of muscular failure the heart rate increased from 85.1±2.07 to 173.4±3.1 beats/minute (p<0.05) along with an increase of R wave from 0.1±0.01 to 0.8±0.21 mV (p<0.05) against the background of a sharp increase of sympathetic effects on the heart. An increase of the duration of the QRS segment was noted from 92.1±2.74 milliseconds to 182.0±9.78 milliseconds (p<0.05), which testified in favor of slowing of the intraventricular conduction. Q wave, reflecting the depolarization of the interventicular septum, deepened from -0.1±0.01 to -0.3±0.05 mV (p<0.05) at the time of muscular failure, which is probably due to the insufficient supply of oxygen-rich blood to the heart muscle. At the time of failure the R-wave amplitude tended to decrease from 2.0±0.1 to 1.6±0.17 mV. S-wave deepening from -0.5±0.07 to -0.9±0.11 mV (p<0.05) at the time of failure and the downward trend of R wave probably reflect a change of the heart's electrical axis [4]. Reduction of the amplitude of T wave from 0.5±0.04 to 0.1±0.1 mV (p<0.05) can be regarded as a sharp enhancement of the sympathetic effects on the heart [5]. By the sixth minute of recovery T wave was almost back to the background. Thus, at the time of failure hemodynamics of the subjects is rapidly activated, sympathetic effects on the heart increase and ECG changes.
Figure 1 shows the mean values of the shifts of ECG parameters with respect to the background at the time of muscular failure during exercise.
It is evident that significant changes of almost all waves and segments of ECG (p<0,05) are noted at the time of failure, but only the values of P, Q, T waves and the QRS segment are beyond the limits of the physiological norm at this time. Probably, the sympathetic effects on the heart were so great at the time of failure that heart rate and, accordingly, impulse frequency in the sinus node of the heart were approaching the maximum, and T wave sharply decreased.
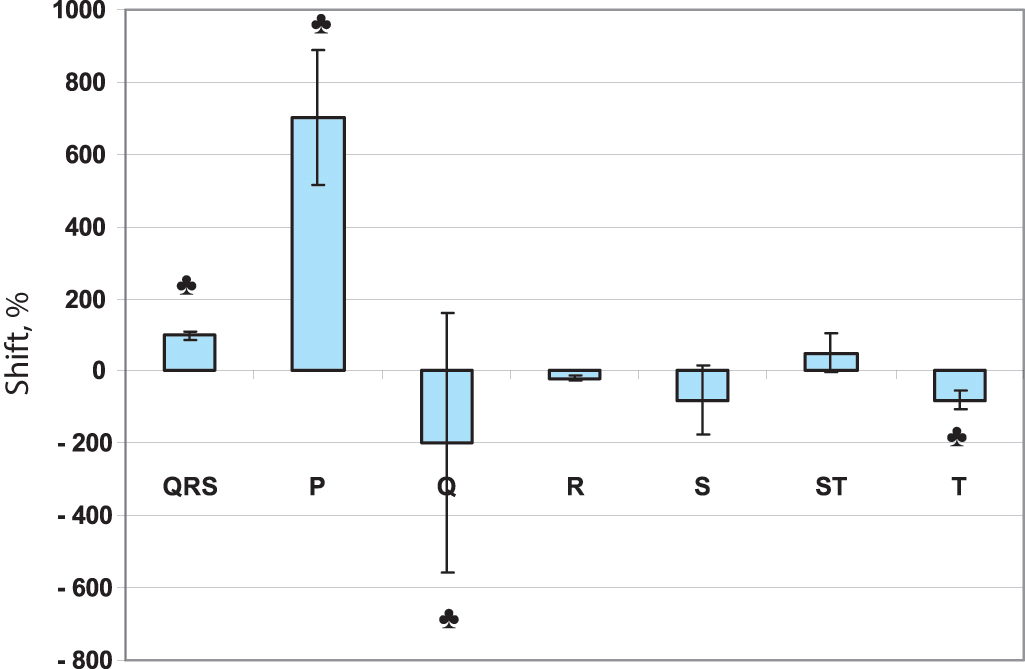
Figure 1. Mean values of the shifts of ECG parameters with respect to the background (%) at the time of muscular failure. Legend: ♣ - at the time of failure the indicator extends beyond the limits of the norm.
It is known that the capabilities of the sinus node in man are limited, and its operation is under strict control of the regulatory systems of the body. The mechanism of slowing down intraventricular conduction is another “controller” of the smooth operation of the heart, and its functioning is reflected in the QRS segment duration. In summary, it should be noted that high heart rate, “extension” beyond the limits of the physiological norm of P, Q, T waves and the QRS segment and exceeding the background level of the minute blood volume by 2-3 times are predictors of endurance exercise on the part of the cardiovascular system during performance to failure. It should be emphasized that after 6 minutes of recovery the Q and T wave values returned to normal, while heart rate, P and the QRS segment just showed a tendency to return to normal range. All this suggests functional changes in the cardiac muscle arising at the time of endurance exercise.
Changes in EMG are also observed at the time of failure. Figure 2 shows the growth dynamics of the number of turns (a) and the average amplitude (Aavg, mV) of EMG at each step of the load. It can be seen that at the step of failure (140 W) the growth of the number of turns of EMG stops, accounted for by a decrease in the pulse frequency of alpha motor neurons. At the same time the average amplitude of EMG also tends to decrease, thus decreasing the contractile ability of the muscles and leading to a decrease in muscle strength. Probably all this indicates muscle fatigue at the time of failure. At the same time the subjects note muscle fatigue in the legs accompanied by a significant reduction in the subjective well-being index from 4.6± 0.1 to 3.8±0.2 points (p<0.05). All this testifies in favor of the subjects having achieved the limits of their physiological capabilities.

Figure 2. Mean values of the number of turns (a) and mean amplitude of EMG (Aavg, mV) of the quadriceps muscle of the right thigh (b) with increasing load (N, W) on a cycle ergometer up to level of failure (140 W). Legend: * - p<0.05 in relation to the background.
Conclusion. The conducted research has revealed that strenuous exercise to failure causes a pronounced increase of the sympathetic effect in the subjects, accompanied by an increase in systolic blood pressure, stroke volume, cardiac output and heart rate. All this is accompanied by an increase of the impulse generation in the sinus node of the heart and a sharp increase of R wave in the ECG, slowing of the intraventricular conduction of impulses and Q and S wave deepening due to the development of motor hypoxia. The T wave, showing the increase of the sympathetic effects on the heart, is reduced. Reduced average amplitude against the background of stabilization of the number of EMG turns indicates muscle fatigue. It should be stressed that at the time of muscular failure the changes of P, Q, T waves and the QRS segment reach the level of marginal compensation, but after 6 minutes of recovery they return to normal.
Thus, all the above confirms the relevance of the conducted research aimed at identifying predictive indicators of endurance exercises in persons engaged in physical culture and sports. The findings can be the ground for the development of individual evaluation criteria of physiological capabilities of athletes and, consequently, contribute to planning of their training and competitive activities.
References
- Karpman, V.L. Dinamika krovoobrashcheniya u sportsmenov (Blood flow dynamics in athletes) / V.L Karpman, B.G. Lyubina. – Moscow: Fizkul’tura i sport, 1982. – 135 P.
- Komantsev, V.N. Metodicheskie osnovy klinicheskoy elektroneyromiografii (Methodical bases of clinical electroneuromyography) / V.N. Komantsev. – St. Petersburg., 2001. – 350 P.
- Pryanishnikova, O.A. Sportivnaya elektroneyromiografiya (Sport electroneuromyography) / O.A. Pryanishnikova, R.M. Gorodnichev, L.R. Gorodnicheva., A.V. Tkachenko // Teoriya i praktika fizicheskoy kultury. – 2005. – № 9. – P. 6.
- Rukovodstvo po kardiologii: prakticheskoe posobie (Cardiological guide: practical guide) / Ed. by V.N. Kovalenko – Kiev: Morion, 2008. – 1424 P.
- Sudakov, K.V. Vegetativnye reaktsii cheloveka pri raznykh rezhimakh teplokholodovykh vozdeystviy v usloviyakh sauny (Human cold- and heat-defense autonomic responses in sauna conditions) / K.V. Sudakov, V.V. Sinichkin, A.A Khasanov // Fiziologiya cheloveka. – 1987. – V. 13. – № 1. – P. 113–119.
Corresponding author: klassina@mail.ru


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE