Implementation of integrated swimming training technique for students with various diseases
Фотографии:

ˑ:
Dr.Med., Associate Professor E.Yu. D'yakova
A.A. Mironov
National Research Tomsk State University, Tomsk
Keywords: exercise therapy, integrated swimming technique, functional state indicators, adaptation
Introduction
As found by regular medical examinations, the numbers of students suffering from inborn or acquired pathologies is on the rise at present [3, Ошибка: источник перёкрестной ссылки не найден]. There are good grounds to rate students as a high-risk health group more susceptible to health problems than other social groups of the same age for the reason that students are more often diagnosed with different somatic disorders and mental diseases [7]. This situation may be largely due to the fact that a human body of that age is still in the process of formation and its adaptation mechanisms are still far from being perfect.
Regular health examinations show that the numbers of students attributed to the basic (healthy) health group fall year-to-year while the preparatory/ special health groups (physically underdeveloped and/or unhealthy students) increase in numbers. On the whole, the lower are the students’ physical development rates the higher are the disease incidence rates. It is the insufficient physical activity of the university students that is believed to be one of the main contributors to this negative trend [8]. Some studies have demonstrated the academic successes being closely correlated with the general functional conditions since every health problem tends to undermine the general workability and contribute to the fatigability of the student [7].
Now it is mandatory for the 1st year students entering National Research Tomsk State University to pass obligatory medical examinations that qualify their health conditions.
As things now stand, it is the exercise therapy (ET) that is considered the main and efficient integrated therapeutic method to cure a wide variety of diseases and prevent their acute attacks. It is since the year of 2010 that the National Research Tomsk State University students diagnosed with serious health disorders have been offered services of specialized ET groups. One of the basic policies of this therapeutic method is to recommend special physical exercises to sick students on condition of their personal serious, active and motivated cooperation in the therapeutic process [Ошибка: источник перёкрестной ссылки не найден]. Therapeutic swimming exercises are now considered one of the top priority methods of the exercise therapy [10].
In view of the fact that most of the unhealthy students referred to the ET groups are poor swimmers, the purpose of our study was to develop and offer an integrated swimming technique to the unhealthy students.
Materials and methods. Subject to the study were the 1st year students of National Research Tomsk State University diagnosed with health disorders and referred to the ET groups. In total 20 volunteers were engaged in the study and evenly split up into Experimental Group and Control Group of 10 people each. The mix of the diagnosed diseases was about the same in both of the groups.
Control Group was subject to ET routine in the gym, with the non-specific health-improving, conditioning and activating exercises dominating in the practices. In addition, sets of special exercises to cure/ mitigate specific diseases were practiced by the Group. The practices were designed to include four phases as required by the relevant valid training regulations, namely: introductory, preparatory, main and final phases.
In the introductory phase, the students measured blood pressure (BP) and heart rate (HR) values and fixed them and other standard health data in the special health record books.
In the preparatory phase, warm-up exercises were done including active walking practices with or without hand movements in combination with respiratory gymnastics.
In the main phase, the practices were 60% based on body conditioning exercises recommendable virtually in every case of health disorder and designed to strengthen main muscle groups and improve physical qualities of the trainees. The remaining 40% of the practice time was given to the disease-specific exercises. Every exercise in the main phase was followed by respiratory practices. The main phase training was free of running, jumping, straining and weight-lifting exercises.
In the final stage, relaxing exercises were made. Motor intensity of the exercises amounted to 60-65%.
In addition to the ET, the Experimental Group students were offered to attend swimming lessons on a voluntary basis. Experimental Group practiced swimming twice a week, each practice being 45 minutes long.
In the introductory phase, the EG students were required to measure BP and HR values to check if they are prepared for the practice. It was followed by warm-up phase when the students performed different preparatory exercises in water. The applied swimming technique was specific in the content of its main phase that was designed with consideration for the specific health disorder of every student and offered special sets of both competitive and therapeutic swimming exercises.
Competitive swimming practices of the course included breaststroke, backstroke, water starts, turnarounds and freestyle. Most of the time was assigned to the breaststroke practices since this style has proved to be the best endurance exercise for this category of trainees. No diving or butterfly practices were accepted for this Group since these movements were considered unsafe for the spine.
The students mastered the competitive swimming techniques in the following sequence:
• Visualize in mind every detail of the movement sequence of the learnt swimming style;
• Make preliminary practical acquaintance with the body positions, breathing sequences and elementary movements and characteristics of the stroke, through stroke imitation and other special exercises in gym and then in water, to master elements of the subject movement sequence; and
• Combine the elementary components of the subject technique and perform them smoothly as an uninterrupted movement sequence.
Every element of the swimming technique was studied in the following succession:
1) Learn and practice the swimming style movements in a gym;
2) Practice the swimming technique using immovable support like a wall of the pool;
3) Practice the swimming technique using buoyant support like plastic board; and
4) Practice the movement sequence in water without support, on the move.
Non-competitive swimming styles were broadly used in the swimming exercises [Ошибка: источник перёкрестной ссылки не найден] including: backstroke legs-forward swim; individual medley; obstacle swim etc.; and the lesson also included special water gymnastics performed in standing position in shallow places or holding the handrails on deep water. In addition, special posture-improvement exercises were applied, including breaststroke on the back holding the board over the head; swimming practice using fins etc. [10]. Ball games and relay competitions were also given significant time in the course.
In the final phase of the swimming lesson, the trainees practiced respiratory and relaxation exercises, water gymnastics and water games.
Overall, the introductory, preparatory and final phases of the swimming lesson accounted for 40% of the total time, and the balance of 60% was taken by the main phase exercises. Motor intensity of the swimming practice totalled 60-65%. Workloads of the health-improvement exercises were designed to raise HR to around 100-150 bpm, with prudential consideration for the individual health restrictions of the trainees.
Both the individual and group practices were used in the swimming lessons to make allowance for the individual needs of the trainees in the context of one or another individual health disorder.
A set of medical tests was used to assess and control influences of the physical work on the trainees and monitor changes in different body systems in the course of the physical exercises. The first medical tests of the subject students were performed in October 2012, at the beginning of the academic year and prior to the ET course. The same health indicators were measured again in April 2013. The tests were performed using the “Valenta” Functional Diagnostics Unit (made by Neo Company Ltd., St. Petersburg, Russia) that produced cardiorhythmographic (CRG) test data and external respiratory function (ERF) test data.
In addition, the "NS-PsychoTest" Psycho-physiological Test Unit (made by "NEURO-SOFT", Ivanovo city, Russia) was used to obtain contact coordination-metric test data and wrist dynamometry test data.
Results and discussion. Medical tests of the 1st year students in 2013 revealed quite high proportions of musculoskeletal and nervous system disorders (38% and 12%, respectively) in this university group (Figure 1). Furthermore, 38% of the tested students were diagnosed with a few health disorders, and 4% were diagnosed with rare diseases like exostosis, different forms of infantile cerebral paralysis etc.
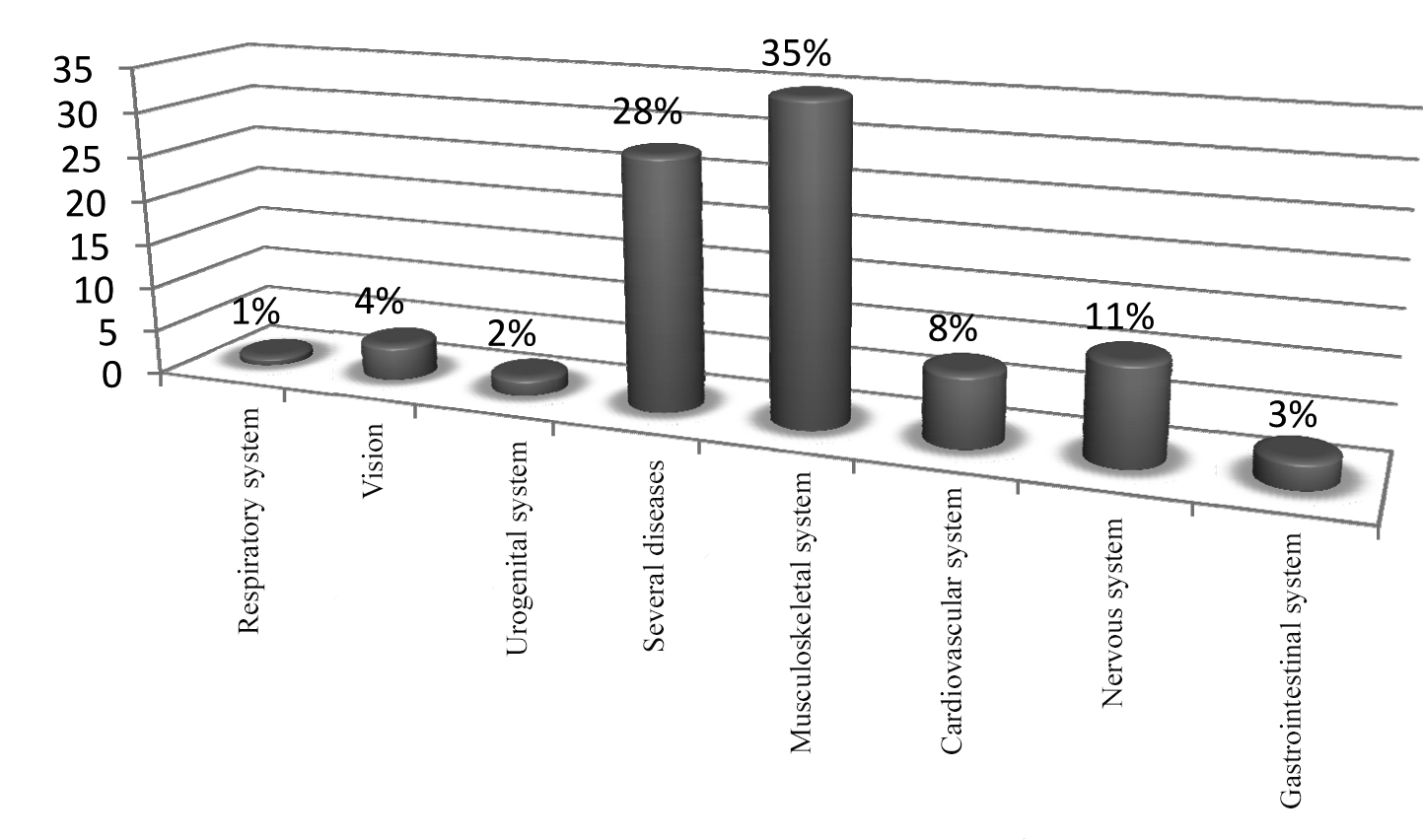
Figure 1. Disease incidence data for ET Group students
The test data were analysed using the “Statistica 10” Windows-based application toolkit from Statsoft. The output data samples showed abnormal distribution of the tested indices, and for this reason the differences of the data samples were valued using the non-parametric rank summation Mann–Whitney test [Ошибка: источник перёкрестной ссылки не найден].
Analysis of the cardiorhythmographic (CRG) test data revealed reliable differences in the following statistical indices of the heart rhythm variations: mathematical expectation, maximum RR value, mean square deviation (MSD) and (SW1+SW2)/FW (vagosympathetic interaction index, Table 1).
Mathematical expectation (M) value is indicative of the final result of the consolidated regulatory impacts on the heart and circulatory system on the whole, and may be considered an equivalent of the mean HR value [11]. At the end of the test, this index was found to grow in the tested students.
Changes in the MSD values may be connected with both the autonomous regulation and the central regulation system (due to sympathetic and parasympathetic impacts on the heart rhythm). Falls in the MSD values are normally indicative of the growing sympathetic regulation process that suppresses the autonomous regulation system activity. Sharp decline of the MSD values is caused by a significant stress of the regulatory systems when the high-level regulatory systems are activated and thereby the autonomous regulation system activity is almost totally suppressed [Ошибка: источник перёкрестной ссылки не найден 9]. Our analysis of the output test data showed some growth of these indices by the end of the year that may be indicative of the stronger autonomous regulation system activity.
The (SW1+SW2)/FW (vagosympathetic interaction index) is indicative of the interaction of the sympathetic and parasympathetic nervous system. Growing indices are normally characteristic of the growing influence of the sympathetic department of the autonomous nervous system (ANS), whilst their decrease is indicative of the growing influence of the parasympathetic department of the ANS [Ошибка: источник перёкрестной ссылки не найден, 6]. The notable fall of these indices (Table 1) is characteristic of the growing contribution of the parasympathetic department of the ANS.
Table 1. Cardiorhythmographic test data for Experimental Group vs. Control Group, %
|
Indices |
EG at the beginning of the year |
EG at the end of the year |
EG index growth, % |
CG index growth, % |
|
Mathematical expectation |
101 |
95 |
-6* |
-4,3 |
|
Maximal RR value |
105 |
91 |
-14 |
-3,4 |
|
MSD |
57 |
67,5 |
10,5* |
-6,5 |
|
(SW1+SW2)/FW |
65 |
33 |
-32* |
-11,7 |
|
*Statistically significant difference in the EG vs. CG indices at the beginning and the end of the academic year, with p<0.05 |
||||
Wrist dynamometry test data with valuations of the nervous process mobility demonstrated statistically reliable growth of the left wrist endurance rates in Experimental Group (Table 2).
Both of the Groups showed some fall of the wrist dynamometry indices by the end of the academic year. This fact may be explained by the growing fatigue due to high physical and mental workloads throughout the academic year that manifests itself in the wrist dynamometry tests.
Table 2. Wrist dynamometry test data for Experimental Group vs. Control Group
|
Indices |
EG at the beginning of the year, Хср±m |
EG at the end of the year, Хср±m |
Growth in the EG, Хср±m |
Growth in the EG, % |
Growth in the CG, % |
|
Maximal muscle strength of the left wrist |
22,8±0,25 |
16,8±0,92 |
-6±0,67 |
-26,3 |
-27,44 |
|
Maximal muscle strength of the right wrist |
25,3±0,42 |
17±1,7 |
-8,3±1,3 |
-33 |
-34,64 |
|
Maximal starting effort of the left wrist |
19,5±1,2 |
15±0,33 |
-4,5±0,87 |
-23,1 |
-24,8 |
|
Maximal starting effort of the right wrist |
19,0±1 |
19,5±1,17 |
-1,5±0,17 |
-7,9 |
-10,5 |
|
Maximal final effort of the left wrist |
15,5±0,5 |
13±0,33 |
-2,5±0,17 |
-13,2 |
-13,6 |
|
Maximal final effort of the right wrist |
15,0±1 |
15±0,7 |
0±0,3 |
0 |
-0,5 |
|
Left wrist endurance index |
81,0±2,33 |
84±0 |
3±2,33 |
3,7* |
2,2 |
|
Right wrist endurance index |
79,5±0,5 |
78,5±0,83 |
-1±0,33 |
-1,3 |
-1,7 |
|
*Statistically significant difference in the EG vs. CG indices at the beginning and the end of the academic year, with p<0.05 |
|||||
Our analysis of the external respiratory function (ERF) and contact coordination-metric test data showed no statistically reliable differences in the relevant test indices for Experimental Group vs. Control Group.
Conclusion
Integrated swimming techniques were developed for application in competitive and therapeutic swimming courses. The new techniques were designed to maximise benefits from water exercises and at the same time prudentially adjust the workloads with consideration for the individual health disorders of the trainees.
Tests of the Experimental Group students showed a significant growth of the adaptation potential of their body systems that gives them the means to adopt more efficiently both to stress situations and physical and emotional workloads in the university studies.
References
- Aikina, L.I. Ispol'zovanie plavaniya v sisteme lechebno-profilakticheskikh uchrezhdeniy (Swimming used in health care facilities) / L.I. Aikina. – Omsk: OGIFK, 2004. – 35 P.
- Baevsky, R.M. Analiz variabel'nosti serdechnogo ritma pri ispol'zovanii razlichnykh elektrokardiograficheskikh sistem (Analysis of heart rate variability using different electrocardiographic systems) / R.M. Baevsky // Vestnik aritmologii. – St. Petersburg, 2001. – № 24. – P. 65–87.
- Bazhukov, S.M. Zdorov'e detey – obshchaya zabota (Children's Health - common concern) / S.M. Bazhukov. – Moscow: UNITI, 2003. – 127 P.
- Berezny, E.A. Prakticheskaya kardioritmografiya (Practical cardiorhythmography) / E.A. Berezny. – St. Petersburg: NEO, 2008. – 93 P.
- Glantz, S. Mediko-biologicheskaya statistika (Biomedical Statistics) / S. Glantz. – Moscow: Praktika, 1999. – 325 P.
- Davlet'yarova, K.V., Kapilevich, L.V. Fiziologicheskie osnovy razvitiya koordinatsii i ravnovesiya u studentov s narusheniyami oporno-dvigatel'nogo apparata (Physiological basics of training of coordination and balance in students with musculoskeletal disorders) / K.V. Davlet'yarova, L.V. Kapilevich // Teoriya i praktika fiz. kul'tury. – 2012. – № 8. – P. 23–26.
- Dedkov, Yu.L. Teoriya i praktika fizicheskoy kul'tury dlya studentov s oslablennym zdorov'em (Theory and practice of physical culture for students with poor health) / Yu.L. Dedkov, V.A. Platonova, E.V. Zefirova. – St. Petersburg: SPbGUITMO, 2008. – 98 P.
- Zaytsev, V.P. Voprosy psikhicheskoy reabilitatsii bol'nykh infarktom miokarda: avtoref. dis. dokt. med. nauk (Issues of mental rehabilitation of patients with myocardial infarction: abstract of doctoral thesis (Med.) / V.P. Zaytsev. – Moscow, 1975. – 25 P.
- Kabachkova, A.V. Reaktsiya regionarnogo krovotoka nizhnikh konechnostey na step-ergometricheskuyu nagruzku u sportsmenov (Response of regional blood flow in legs to step-ergometer exercise in athletes) / A.V. Kabachkova, Ju.S. Frolova, L.V. Kapilevich // Teoriya i praktika fiz. kul'tury. – 2014. – № 10. – P. 56–58.
- Medvedev, B.A. Skolioz i osteokhondroz: profilaktika i lechenie (Scoliosis and osteochondrosis: prevention and treatment) / B.A. Medvedev. – Rostov n/D: Fenix, 2004. – 192 P.
- Mikhaylov, V.M. Variabel'nost' ritma serdca. Opyt prakticheskogo primeneniya (Heart rate variability. Practical experience) / V.M. Mikhaylov. – Ivanovo: NEO, 2000. – 35 P.
- Sadykov, R.I. Ozdorovitel'no-reabilitatsionnaya fizicheskaya kul'tura studentov, otnesennykh po sostoyaniyu zdorov'ya k spetsial'nym meditsinskim gruppam v vysshey shkole (Recreational and rehabilitative physical culture for students referred to special medical group in higher school due to health [electronic resource]: South Ural State University). Available at: http://conf-v.narod.ru/s2d53.htm (date of access: 15.12.2014)
- Teoriya i metodika obucheniya plavaniyu studentov vysshikh uchebnykh zavedeniy: uchebno-metod. posobie (Theory and methodology of swimming training for university students: study guide) / M.G. Nepochatykh, V.A. Bogdanova, K.S. Labzo et al. – St. Petersburg: Pub. h-se of SPbSUEF, 2009.
Corresponding author: kapil@yandex.ru


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE