Biomechanical characteristics of walking of patients with cerebral palsy
Фотографии:

ˑ:
Ph.D., Associate Professor K.V. Davlet'yarova2
Postgraduate student S.D. Korshunov2
Dr.Med, Professor L.V. Kapilevich1
Recreation therapist A.V. Rogov2
1National Research Tomsk State University, Tomsk
2Tomsk Polytechnic University, Tomsk
Keywords: walking, locomotions, movement disorders, biomechanics, antagonistic muscles.
Introduction. Movement is among the main physiological components of the normal formation and development of the body in children. It contributes to the development of all the areas of the cerebral cortex, intercentral connections coordination, correction and compensation of shortcomings in physical and mental development as well as to the formation of motor interaction of analyzer systems and cognitive processes [7, 9]. Movement is a necessary condition of life support of the body, as well as the means and method of maintaining its performance.
Cerebral palsy (CP) is a severe neurological disease that substantially limits vital activity of a child. First of all, it leads to movement disorders [2, 5]. Accordingly, an important rehabilitation area for such children is maximum recovery of motor skills that can be implemented on the basis of studying the biomechanics of movement disorders [1, 8].
Biomechanical locomotion disorders are characterized by pathological stereotypes of posture and walking. They are formed on the basis of tonic reflexes that maintain their pathological activity [3, 4, 6]. At the same time the existing pathological movement stereotypes can be the basis for the formation of new motor skills, which will lead to an increase in the motor activity of a child and provide a good rehabilitation effect.
The purpose of the research is to study the biochemical characteristics of walking of the patients with cerebral palsy.
Materials and methods. To address the goal 20 children (12 boys and 8 girls) aged from 8 to 12 years old were examined. All the children suffered from cerebral palsy in the spastic diplegia from and were undergoing treatment and adaptation in the regional state institution «Rehabilitation center for children and adolescents with impairments» (CATU, Seversk). There were 10 children (6 boys and 4 girls) of the same age in the control group. All the subjects performed walking on a treadmill in three positions: on a flat surface and uphill and downhill at 8 degrees. The Motion Tracking method was used for analyzing the orientation of body parts, their location in space and the way they are related to the support. Movements of the body parts were recorded by a video camera Vision Research Phantom Mire eX2. The shooting was done at a speed of 100 frames per second. The obtained data were processes and analyzed in the Star Trace Tracker 1.1 Video Motion® program.
Results and discussion. Based on the results we can identify the main differences in the construction of a dynamic walking stereotype of children with cerebral palsy. The dynamics of the angles in the joints of the lower extremities was not qualitatively different (Figure 1). At the same time the angle of flexion of the hip joint in the patients with cerebral palsy was slightly lower in the first half of a step, but turned out to be considerably higher in the second half. The movement in the hip joint has alternating ceding and overcoming character. Patients with cerebral palsy have a weakened ceding phase and a considerable increase in the overcoming phase.
However, significant differences were observed between the groups in terms of the angular velocities in the joints (Figure 2). The center of gravity of a healthy child moved forward and up predominantly in the first half of a step. The movement of children with impairments began with moving downward, the main move forward occurred in the second phase of a step and was accompanied by some move upward. In children with cerebral palsy angular velocities of movement in the knee and ankle joints have extremes in the same phases, but all the extreme values are shifted to positive angles, reflecting mainly a bent leg position.
Reduction of the value of angular velocity in the knee joint of the patients with cerebral palsy is associated with a decrease in the ability of the central nervous system to coordinate the tone of antagonistic muscles. Pelvic rotation is an important part of the mechanism of shifting of the whole body from one foot to another and the mechanism ensuring the leg movement when walking. In children with cerebral palsy the phase structure of this movement changes dramatically (Figure 2). We can assume that these changes are of compensatory nature, compensating for the limited mobility in the knee joints.
Remarkable differences between healthy children and those with cerebral palsy were found in the function of the upper extremities. Children with impairments are first of all characterized by higher values of the angles in the shoulder joint and lower values in the elbow joint throughout a step (Figure 1). Elbow and wrist movements of healthy children matched in phase both horizontally and vertically. The beginning of a step was accompanied by a hand movement forward and upward, during the third-fifth phases - backward and downward, then up again. In case of children with cerebral palsy horizontal elbow and wrist movements took place in reverse phase - a step began with an elbow movement backward, and a wrist movement forward. In the third-fifth phases the directions changed: the elbow moved forward, and the wrist - backward. In children with impairments we saw slow wrist movements up and down in the vertical plane.
Conclusion. The main differences of the dynamic stereotype of walking of children with cerebral palsy are delayed travel of the center of gravity forward (it takes place in the second half of a step) and disorganization of the lower extremity movements (especially knees) in the vertical plane. The prevailing adduction-flexion position of legs during the locomotor cycle associated with the restriction of movements in the hip joint, is made up by more intensive body-rocking, weakened activity in the rear push phase and its sharp increase in the fourth phase. Changes in the structure of shoulder girdle and arm movement can be considered as compensatory: vertical shoulder movements adjust to those of the center of gravity while remaining in the reversed phase to the latter. A mismatch of the elbow and wrist movements takes place - they move in the reversed phase too. We can assume that in case of patients with cerebral palsy simultaneous activity of extensor and flexor muscles is not incidental, but the key feature of the locomotion control, being both a manifestation of pathological disorders and a compensatory mechanism.
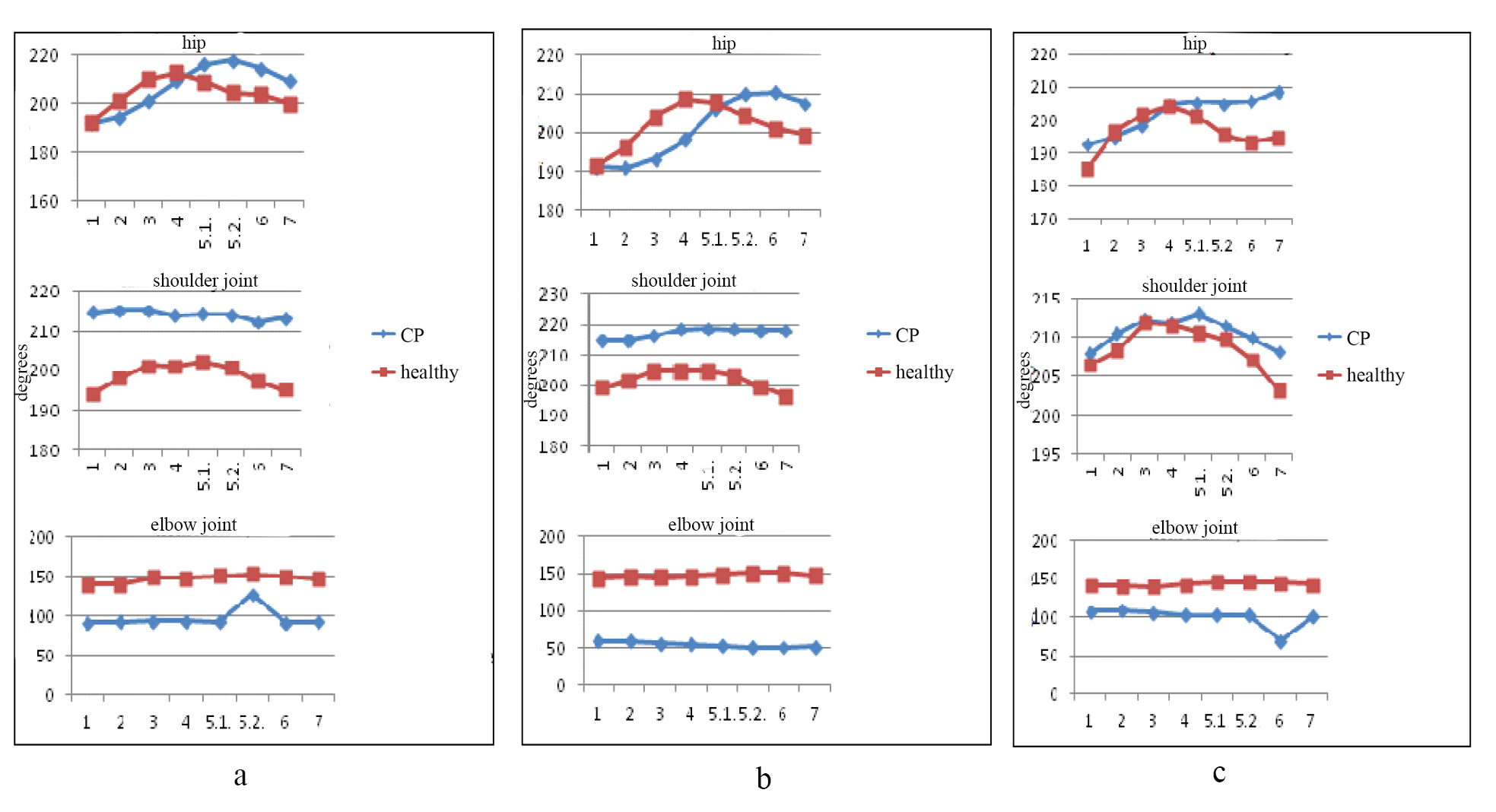
Figure 1. Values of angles in the joints of the upper and lower extremities while walking:
a - uphill, b – on a flat surface, c - downhill
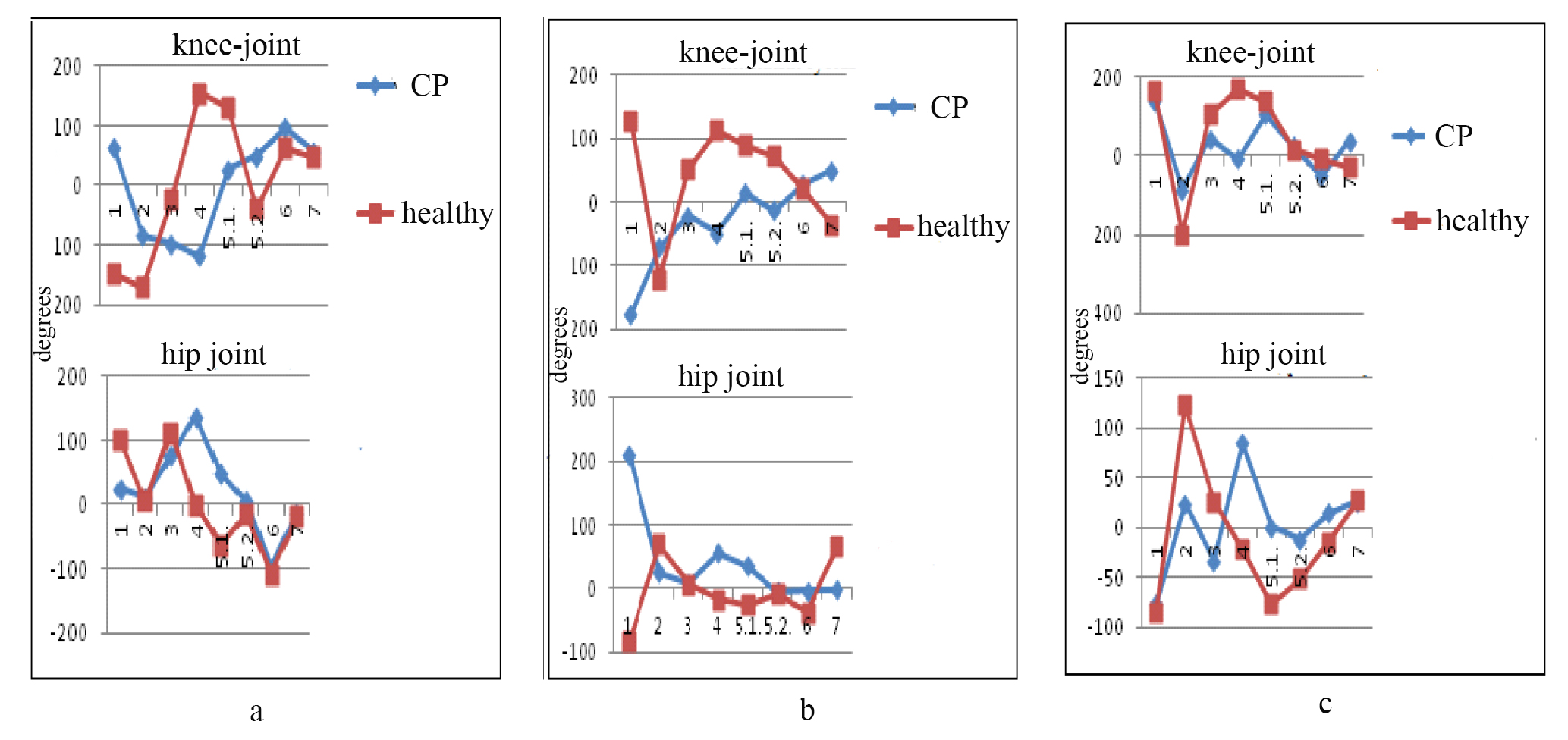
Figure 2. Values of angular velocities in the joints of the lower extremities while walking:
a - uphill, b – on a flat surface, c - downhill
References
- Dubrovskiy, V.I. Patologicheskaya biomekhanika (Abnormal biomechanics) // Biomekhanika: uchebnik dlya sred. i vyssh. ucheb. zavedeniy (Biomechanics: textbook for second. and higher. educ. institutions) / V.I. Dubrovskiy, V.N. Fedorova. – Moscow: VLADOS-PRESS, 2003. – P. 591–628.
- D'yakova, E.Yu. Lechebnaya fizicheskaya kul'tura kak forma realizatsii uchebnogo protsessa po fizicheskomu vospitaniyu studentov (Physical therapy as a form of implementation of educational process on physical education of students) / E.Yu. D'yakova, L.V. Kapilevich, O.Kh. Boltaeva et al. // Teoriya i praktika fiz. kul'tury. – 2010. – № 10. – P. 62–63.
- Kapilevich, L.V. Fiziologicheskiy kontrol' tekhnicheskoy podgotovlennosti sportsmenov (Physiological control of technical fitness of athletes) / L.V. Kapilevich // Teoriya i praktika fiz. kul'tury. – 2010. – № 11. – P. 12–15.
- Kashuba, V.A. Komp'yuternaya diagnostika oporno-dvigatel'noy funktsii cheloveka (Computer diagnostics of locomotor functions in man) / V.A. Kashuba, K.N. Sergienko, D.N. Valikov // Fizicheskoe vospitanie studentov tvorcheskikh spetsial'nostey. – Kharkov: HHPI, – 2002. – № 1. – S. 11–16.
- Osokin, V.V. Evolyutsiya predstavleniy o detskom tserebral'nom paraliche (Evolution of cerebral palsy related ideas) / V.V. Osokin // Sovremennaya nauka: aktual'nye problemy i puti ikh resheniya. – 2014. – № 9.
- Potovskaya, E.S. Vospitanie silovyh sposobnostey i vynoslivosti u studentok (Training of strength abilities and endurance in female students) / E.S. Potovskaya, V.G. Shil'ko // Teoriya i praktika fiz. kul'tury. – 2013. – № 4. – P. 20–23.
- Imms, C. Children with cerebral palsy participate: a review of the literature // Disabil. Rehabil. 2008. Vol. 11/30;30(24). P. 1867–1884.
- Lusardi, M.M. Orthotics and Prosthetics in Rehabilitation. Elsevier Corp. / M.M. Lusardi, C.C. Nielsen – 2007. – 904 P.
- Sharma, R. An Objective Approach for Assessment of Balance Disorders and Role of Visual Biofeedback Training in the Treatment of Balance Disorders//Indian J. of Physical Medicine and Rehabilitation. 2001. V. 12. P. 25-30.
Corresponding author: kapil@yandex.ru


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE