Criteria and Methods of Human Motor Activity (Overview)
Фотографии:

ˑ:
V.I. Lyakh, professor, Dr.Hab.
Academia of Physical Education, Krakow
O.G. Rumba, senior lecturer, Dr.Hab.
National Research Belgorod State University, Belgorod
A.A. Gorelov, professor, Dr.Hab.
Institute of Socialization and Education of Russian Academy of Education, Moscow
Key words: motor activity (MA); indicators, criteria, methods of estimation of MA, classification of methods, current problems.
The relevance of searching for good quality methods, technologies and instruments of measurement of motor activity (MA) is caused, first of all, by the close correlation between MA, health status and physical fitness [7, 18, 22, 27, 1, 2, 3]. It concerns both individual case and assessment of MA of the subjects of specific age-sex groups.
Scientists from all over the world have worked and keep working at the issue of development of valid methods for the estimation of human MA [5, 16, 17, 19, 23, 25, 26, 30, 31, 20]. With regard to this issue, there are also fundamental reviews [5, 7, 9, 16, 17, 19, 20, 26, 31], the authors of which try to systematize the research methods and criteria of MA, discuss problems and difficulties, and argue about the prospects for the further development of such a highly challenging for science - and important in practice - problem.
The purpose of this review article is to generalize and analyze the scientific information on the research methods and criteria of human MA as well as to identify the problems and difficulties that have to be overcome in order to use these findings in independent researches.
Problems and difficulties. The determination of significant criteria regarding the techniques and instruments used for this purpose appears as one of the basic methodological problems of the research of MA. It is commonly known, that the following criteria are considered the most important ones: reliability, validity, standardization, objectivity and efficiency of measurement procedures. If repeated research of MA using a certain technique or instruments does not give rise to great difficulties, the assessment of the method's validity appears to be a methodologically complex task. The reason for this is the lack of readily available research techniques and instruments that would meet the criteria of the so-called "gold standard". It is also stressed that the use in the validity's assessment of the research instruments as to the statistical values of the correlation coefficient of the results, obtained using two or more methods, is unreliable due to an error in the measurements of each of them [31]. In this regard, it is recommended to rely upon at least two or more techniques at the same time [14, 31].
When it comes to objective research of the human MA, the second issue is the necessity to take into account the following elements:
- age and sex of the subjects;
- type of MA (professional, sports, recreational, health-centered, based on the level of determined motor skills);
- goal of classes (health-improving, recreational, sports, practical);
- time of year and environmental conditions (temperature, air humidity, landscape);
- demographic indicators (race, social origin, environmental living conditions);
- objectives (motives) of classes [20, 31].
The third issue as to the specificity of the measurement of MA results from the difficulty in defining the very concept of "motor activity." Despite the fact that this term is widely known and used, it is not an easy one to define [31]. More often than not, the term "MA" is understood as any body movement performed by skeletal muscles and associated with energy expenditure at a level higher than metabolism at rest [4, 7, 8]. From the perspective of physiology, MA strikes as being part of the overall energy consumption, concomitantly with metabolism at rest, a specific dynamic action of food and the body’s growth process. If we see things through a behavioural perspective, then it is a volitional motor act in extension or an exertion of force against external forces.
Hence, given the fact that MA consists of a bunch of simultaneously performed processes, which may be characterized by various methods, the assessment of the criterion validity of the research method of MA, especially when it comes to large populations, can cause great difficulties [11].
Indicators and criteria of MA
The amount of consumed energy (energy expenditure - EE) appears to be one of the best indicators of MA [14], although it is emphasized [19] that EE is not synonymous with MA. As a matter of fact, the MA of varying intensity and capacity may have an equal-to-EE value, although, in this case, it leads to a completely different set of recreational effects [19]. Therefore, if we wish to assess the effect that MA has on health, not only we must pay attention to the amount of consumed energy during its flow, but also we have to take the form, the intensity, the duration and the frequency of the performed MA into account [7, 8, 31]. Furthermore, we should not forget about the impact of the external environment, the mental set and objectives of the attempted MA, which can affect its physiological effects to a great extent [19].
The amount of lost energy (EE), just like the criteria of the level of MA, is measured in the traditional unit of heat "kilocalorie" (kcal) or, in accordance with the SI system, in the unit of functioning and energy "joule" (J). Therewithal, 1 kcal = 4.186 kJ, 1kJ = 0.239 kcal [31].
The amount of consumed oxygen per kg of the body mass in time units is also used as an EE measuring element, as the EE value is determined by the body mass value [19]. Hence the value of the consumed energy most commonly results from the accordance with a person's body mass, or with the help of the multiplicity of MET (1 MET is equal to the amount of energy consumed [EE] at rest). It is accepted that the EE at rest in adults is approximately 4.2 kJ (1 kcal) x kg-1 x h-1 or 3,5 ml О2 kg-1 x min-1 [31]. Based on MET units, a large number of classifications of various forms of MA was developed and recommended to practices: recreational, sports, professional, self-service [1, 15, 31, 20]. MET units are also used in the systematization of the intensity of MA [31]. An example of this classification is given in Table.
Table. Classification of various forms of motor activity on MET units [15]
|
Intensity of effort (MET) |
Type of motor activity |
|
2.5 |
Walking at 3-3.2 km/h on flat surface; billiard |
|
3.0 |
Walking at 4 km/h; descending stairs, downhill walking at 4 km/h, riding on an ergometer at 50 watts; skittles; non-professional volleyball, 6-on-6; dancing |
|
3.5 |
Walking at 4.8 km/h; recreational swimming (100m in 3min); rowing ergometer at 50 watts; walk with a dog |
|
4.0 |
Walking at 5.5 km/h; stretching; hatha yoga; recreational bicycle riding at less than 16 km/h; horse riding; table tennis |
|
4.5 |
Recreational badminton; walking at 6.5 km/h; dancing |
|
5.0 |
Cycloergometer; work in the garden; alpine skiing (with low strain); fishing |
|
5.5 |
Cycloergometer at 100 watts; disco/folk dancing |
|
6.0 |
Uphill walking 5.5 km/h; walking with travel gear; strength training; bicycle riding at speeds of 16-20 km/h; slalom skiing (moderate strain); swimming (100 m / 2 min); swimming in a lake/ the sea; boxing; fighting (up to 5 min); aerobics; modern ballet; twist dancing |
|
6.5 |
Military march |
|
7.0 |
Jogging; alpinism with extra weight of up to 4 kg; cycloergometer at 150 watts; rowing ergometer at 100 watts; cross-country skiing at 4km/h with low strain; ice skating, tennis |
|
7.5 |
Alpinism with extra weight of 4.5-9 kg |
|
8.0 |
Running 8 km/h (1 km / 7.5 min); alpinism with extra weight of 10-20 kg; bicycling at 20-22 km/h; cross-country skiing t 6.5-8 km/h; swimming (100 m / 1 min 45 sec); basketball, football; long jumps; water volleyball |
|
8.5 |
Rowing ergometer at 150 watts (heavy load) |
|
9.0 |
Running at 9 km/h (1 km / 6 min 40 sec); ice skating (at speeds of more than 15 km/h); figure skating; cross-country skiing at 8-13 km/h |
|
10.0 |
Running at 10 km/h (1 km / 6 min); bicycling at 22-25 km/h; swimming (100 m / 1 min 20 - 1 min 30 sec); Asian martial arts; rowing |
|
10.5 |
Cycloergometer at 200 watts (heavy exertion) |
|
11.0 |
Running at 12 km/h (1 km / 5 min 30 sec); butterfly swimming |
|
12.0 |
Running at 12 km/h (1 km / 5 min); rowing ergometer at 200 watts; bicycling at 25-30 km/h |
|
12.5 |
Cycloergometer at 250 watts (extremely high load) |
|
13.5 |
Running at 13 km/h (1 km / 4 min 40 sec); cross-country skiing at more than 13 km/h |
|
15.0 |
Running at 14.5 km/h (1 km / 4 min 10 sec); descending stairs running |
|
16.0 |
Running at 16 km/h (1 km / 3 min 45 sec); bicycling at more than 32 km/h |
Methods of MA assessment. One of the most common classifications of MA research methods is presented in Fig. 1. As follows, the mentioned authors divide MA measurement methods into objective and subjective. According to the prevailing view [16], only the first ones can be considered, in every sense of it, as MA measurement methods, given the fact that the measuring technique used in this case is based on the precise measurement (record keeping, monitoring) of the organism's physiological reactions to physical load and determination of the kinematic parameters of the performed movements. In this regard, the accuracy of the MA measurement, with the help of various measurement techniques and their use in large-scale studies, is shown in Fig. 2.
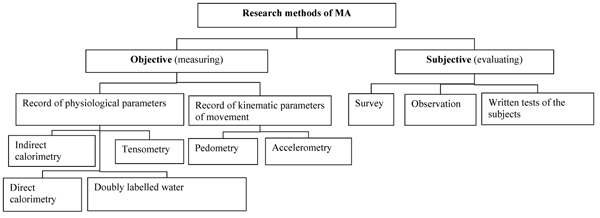
Fig. 1. Research methods of MA [16,20]
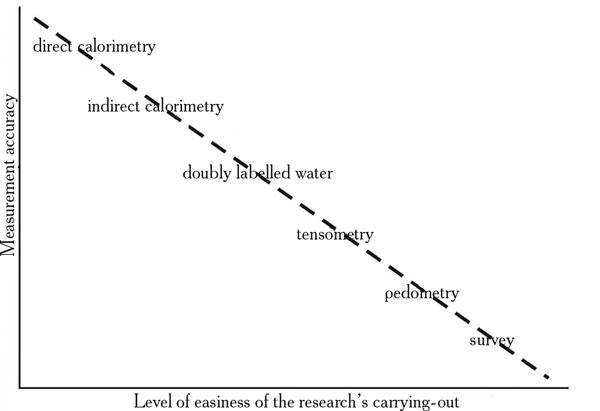
Fig. 2. Hierarchy of measurement and evaluation techniques of MA depending on their accuracy and applicability in large-scale studies (Eklund, 2004; [20])
The final results of the physiological and biomechanical studies come in the form of energy cost units which, as it was observed, are recognized as the best measuring elements of the human MA. These research techniques allow the obtainment of indirect MA results, recalculated on the basis of recorded parameters in kilocalories. Hence, the presented classification of the measuring techniques of MA is based on the record keeping of the physiological and kinematic parameters of movement [20].
The subjective methods of the MA assessment are based on various forms of the test subjects' self-assessment. The research techniques used for these purposes are designed on the basis of the calculation procedure of the collected information in units with costs in calories.
The objective methods are common in natural sciences, whereas the subjective ones in humanities sciences [20].
Characteristics of the selected research methods of MA.
The objective measurement techniques of MA, on the basis of physiological parameters, settle for the determination of the MA's amount and intensity by means of the record keeping of an organism's physiological reactions to a certain load (change in body temperature, HR, amount of oxygen and carbon dioxide inhaled and exhaled, etc.). The ones standing out, as shown in Fig.1, are direct and indirect calorimetry as well as doubly labelled water.
In direct calorimetry, the measurement is carried out in a "calorimetric" chamber or a special outfit coupled with a system of tubes through which water flows. In such a chamber or outfit, a subject performs a particular exercise, for example on a cycle ergometer, emitting - as a result of the metabolic load - heat which increases the temperature in the tubes. Based on the differences of the pre and post-exercise water's temperature, the amount of the subject's emitted heat is estimated (in calories). The low probability of an error in the measurement's accuracy (approximately 1%) is the advantage of this technique, while the disadvantageous features seem to be the long time during which a subject remains in vitro as well as the burdensome measurement procedures [31, 12, 20].
Indirect calorimetry. This technique is based on the correlation between the amount of oxygen (O2) used during the exercise and the amount of carbon dioxide (CO2) emitted. The measurement of the oxygen consumption and carbon dioxide emission is carried out using special actuators and mouthpieces connected with portable gas analysers while breathing. By knowing the amount of O2 consumed and CO2 emitted, it is possible to indirectly estimate the value of energy expenditure (ЕЕ). This method of estimating the MA level is especially useful for the assessment of the energy cost of aerobic-related efforts [16, 20]. Thanks to the same-with-the-previous-case high measurement accuracy, both of the above-described techniques can be considered to determine the validity of other measurement methods of human MA [31].
Doubly labelled water. The essence of this technique is limited to the restoration of the original composition of the water's isotopes during the nutrient metabolism. The subject drinks water designated by isotopes of hydrogen (deuter 2H) and oxygen (18O). The isotope of hydrogen cleans the organism in the form of water vapour through the urine, sweat and exhaled air. The designated oxygen is released from the organism also aquatically (H218O), and even as carbon dioxide (C18 O2). Based on the knowledge of the differences in the emission of both isotopes with the use of the corresponding equations, the amount of CO2 in human organism is calculated and, with the value of respiratory quotient (RQ) known, the amount of consumed oxygen is estimated. Implicitly, this helps to determine energy expenditure during exercise. It is evidenced that, for this measurement technique's accurate EE measurement, a week of observation is enough for children, whereas two are needed for adults [31, 16, 20]. The DLW method is recognized as the best amongst the renowned techniques (ways) of EE estimation. Therefore, it is taken as a "gold standard", given its high measurement quality (validity, reliability). However, it cannot be used in population studies due to the high cost of this measurement procedure and its time-consuming nature [20].
Heart rate monitoring (HR). HR recording devices are used for this purpose; pulsometers used, for example, in the programming and monitoring of training load in sport and recreation. The capability of estimating the energy expenditure during MA on the basis of HR derives from the existent high correlation between the HR value and the amount of consumed oxygen. However, the HR values (bpm), consistent with the amount of maximal oxygen consumption (ml/kg/min), have an individual character, since they depend on the functionality level of the cardiovascular and respiratory systems. Thus, the estimation of the actual EE indicator of a specific individual requires the prior estimation of physical performance (maximal oxygen consumption) in vitro.
The cutting-edge pulsometers (sport-testers) are based on the digital technology that enables not only to measure HR, but also covered distance, number of made steps, acceleration and ambient temperature. Those devices allow the HR record-keeping in predetermined time intervals, for example, in five, ten and sixty-minute periods, thus the performed MA can be determined. The interface enables the data transfer from the sport-tester to a computer which, with the presence of a relevant software, provides the further analysis of the results. According to professor Scheklitsky [31], a reliable and valid estimation of daily MA can be taken on the basis of a continuous 4-5 days long HR monitoring, taking into account holidays and weekends. But, what strikes as being the pulsometers' greatest advantage is their ability to measure the changing intensity of the performed MA during aerobic exercises. Their disadvantage lies in the fact that they are unsuitable for the estimation of MA in anaerobic exercises [30].
MA measuring techniques based on kinematic parameters of movement. The use of such a type of measurement is based on the rectification and the record-keeping of the kinematic parameters of movement, as well as the based-on-them calculation of EE. Various mechanical or electronic forms of record-keeping of the flowing movements' parameters are applied for this purpose, enabling the calculation of the body acceleration value as well as the number of steps. Monitor sensors, pedometers and accelerometers are the devices used for this purpose [21].
Pedometers are, in substance, small-sized mechanical or electronic devices fixed at the hip level or at the ankle of the lower limb, which keep record of the taken steps. In addition, some of them can be used to estimate covered distance and calculate the energy expenditure of the performed MA as well. The information about the length of a typical step of a subject as well as his/her body mass is stored in the memory of these devices. What is considered as the main disadvantage of pedometers is their inability to recognize intensity of exercise; for example, the intensity of the varying-in-time walking and jogging, performed with dissimilar speed. Another disadvantage of these types of devices seems to be the record-keeping of the body movement only in the frontal plane, as well as the inability to record strong vibrations that occur, for instance, when jumping or bouncing in place, which are recorded as steps. The most reliable results regarding the use of pedometers are obtained by walking of moderate intensity; 80m/min [20]. Accessibility, low cost and easy usage are considered as some of their advantages [20].
Accelerometers. During acceleration, energy is delivered from the muscles, depending on the exertion's intensity. Accelerometers are based on this principle. These are small electronic devices fixed mostly at the thigh level, not limiting the amplitude of the performed movements. At first, there were only single axis accelerometers; for example, caltrac monitor of the firm Muscle Dynamik [20]. Nowadays, multi-axial accelerometers have made their appearance, which can be used to measure the acceleration in the frontal, sagittal or vertical planes (for instance, ActiGraph GT3Xplus; www.theactigraph.com), as well as the movement of the whole body or its individual parts by means of electromechanical, optical or piezoelectric sensors [20]. For example, with the help of new-generation accelerometers, the record-keeping of acceleration of the whole body and its separate parts can be achieved, as can also be the number of taken steps, length of the covered distance, sitting and lying time, walking and jogging time and the number of postural changes, e.x. from the lying position to the sitting one and from the sitting position to the standing one. Other types of accelerometers (for instance, SenseWear Armand; www.templehe-althcare.wordpress.com) monitor changes in the body heat during physical load. The most significant advantages of these objective MA measurement techniques include: the ability of the exertion time's record-keeping in various zones of intensity as well as the estimation of this exertion's energy cost; the ability of using them in field conditions; the realization of measurement in a few hours; the conversion of the recorded data, using a computer, to the information necessary for the researcher. The adequate reliability and validity of the cutting-edge accelerometers in scientific researches are also completely ascertained [20].
At first, when it comes to human MA studies, only subjective methods and techniques for its evaluation were used, relatively easy as to their carrying-out and not time-consuming. Because of these reasons, these methods still occupy a large place in the researches of scientists of various countries, including Russia.
The subjective methods (techniques) of the human MA research are the following:
1) diagnostic probing and control, built on the basis of relevant surveys and questionnaires filled up by the subject on his/her own (self-assessment) or the researcher (through interviewing);
2) descriptive methods, among which the following stand out: a) direct observation (by an experimenter); b) indirect observation (using audio-video); c) keeping of a control diary which includes all the actions performed by a subject during a predetermined time period.
No further detailed information on the subject of the analysis of the MA research subjective methods is provided in our survey because of the undoubtedly high publicity and prevalence of these methods in the researches of Russian scientists. We refer an interested reader to surveys [9, 18, 20, 23, 24, 27, 28, 29, 31, 32] as well.
Conclusion. The conducted analysis of the problems of human MA research showed that, on the one hand, objective methods allow the accurate evaluation of various MA parameters but, on the other hand, they cannot be used, at this point, in population-based studies, which enable the creation of programmes for the popularization of MA in various social groups. As to the future, according to experts [20], regarding the measurement of MA, first and foremost, it's necessary to use measurement devices allowing the simultaneous record-keeping of both the physiological and the biomechanical indicators of performed MA. Such efforts have already been seen through in success. For example, the device has been built - ActiTrainer (www.theactigraph.com) - which combines the functions of a tensometer and an accelerometer [20]. Secondly, we must not count out the subjective methods of MA measurement, for example, standardized questionnaires, especially if they meet the criteria of objectiveness and validity and are carried out in concordance with the norms, inclusive of the energy expenditure (kcal) during the performance of all possible movements (Table 1). Thirdly, it is necessary to organize studies for the assessment of the validity and reliability of the subjective methods of the MA measurement, based on the objective criteria and methods of its estimation.
References
- Kolosov, V.P. Physical activity and health of young students / V.P. Kolosov, A.V. Leyfa, Yu.M. Prel’man, K.N. Sizonenko. – Vladivostok: Dal’nauka, 2007. – 221 P. (In Russian)
- Polievsky, S.A. Stimulation of motor activity / S.A. Polievsky. – Moscow: Fizicheskaya kultura, 2006. – 254 P. (In Russian)
- Rumba, O.G. System mechanisms of regulation of motor activity of students from special medical groups: monograph. – Belgorod: LitKaraVan, 2011. – 460 P. (In Russian)
- Anshel M.H., Freedson P., Hamill J., Haywood K., Horvat M., Plowman S.A. Dictionary of the sport and exercise sciences. Human Kinetics Books Champaign, Illinois 1991.
- Baranowski T., Bouchard C., Bar-Or O. et. al. Assessment, prevalence and cardiovascular benefits of physical activity and fitness in youth. Medicine & Science in Sport & Exercise, 1992, 24 (supp. 6), 237-247.
- Biernat E., Stupnicki R., Lebiedziński B., Janczewska L. Assessment of physical activity by IPAQ questionnaire. Physical Education and Sport, 2008, 52, 46-52.
- Bouchard C., Shephard R.J. Physical activity, fitness and health. The model and key concepts (W:) Bouchard C., Shephard R.J. Stephens T. (red.). Physical activity, fitness and health. International proceedings and consensus statement. Human Kinetics Publishers, Champaign 1994, 77-88.
- Bouchard C., Shephard R.J., Stephens T. (red.). Physical Activity, fitness and health. International proceedings and consensus statement. Human Kinetics Publishers, Champaign 1994.
- Craig C.L., Marshall A.L., Sjöstrom M. et. al. International Physical Activity Questionnaire: 12-country reliability and validity. Medicine & Science in Sports & Exercise, 2003, 35 (8), 1381-1395.
- Haskell W.L. Health consequences of physical activity: understanding and challenges regarding dose – response. “Med. Sci. Sports Exerc”, 1994, 31, 629-631.
- Haskell W.L., Yee M.C., Evans A., Irby P.J. Simultaneous measurement of heart rate and body motion to quantitate physical activity. “Med. Sci. Sports Exerc”, 1993, 25, 109-115.
- Haugen H.A., Chan L.N. Indirect calorimetry: A practical guide for clinicians. Nutrition in Clinical Practice, 2007, 22 (4), 377-388.
- Jegier A. (red.). Aktywność ruchowa w zdrowiu i chorobie. Medicina Sportiva, 2004, 8 (suppl.), 1-79.
- Kemper H.C.G. (red.). The Amsterdam growths study. A longitudinal analysis of health, fitness, and life style. Human Kinetics Publishers. Champaign 1995.
- Kuński H. Trening zdrowotny osób dorosłych. Przewodnik lekarza i trenera. MedSportPress. Warszawa, 2003.
- Lipert A., Jegier A. Metody pomiaru aktywności ruchowej człowieka. Medycyna Sportowa, 2009, 25 (6), 155-168.
- Melanson Jr E.L., Freedson P.S. Physical activity assessment: A review of methods. Critical Reviews in Food Science and Nutrition, 1996, 36 (5), 385-396.
- Moddison R., Mhurchu C.N., Jiang Y. et. al. International physical activity questionnaire (IPAQ) and New Zeland physical activity questionnaire (NZPAQ): A doubly labelled water validation. International Journal of Behavioral Nutrition and Physical Activity, 2007, 4, 62.
- Montoye H.J., Kemper H.C.G., Saris W.H.M., Washburn R.A. Measuring physical activity and energy expenditure. Human Kinetics. Champaign 1996.
- Mynarski W., Rozpara M., Królikowska B., Puciato D., Graczykowska B. Jakościowe i ilościowe aspekty aktywności ruchowej. Studia i Monografie, 313, Politechnika Opolska, 2012.
- Osiński W. Antropomotoryka. AWF, Poznań, 2003.
- Pate R.R. Physical activity and health: dose – response issues. “Res. Quart. Exer. Sport, 1995, 66, 313-317.
- Plewa M. Wybrane metody pomiaru aktywności fizycznej w otyłości. AWF, Katowice, 2008.
- Rütten A., Ziemainz H., Schena F. et.al. Using different physical activity measurements in eight European countries. Results of the European Physical Activity Surveillance System (EUPASS) time series survey. Public Health Nutrition, 2003, 6 (4), 371-376.
- Schneider P.L., Crouter S.E., Basset D.R. Pedometer measures of free-living physical activity: Comparison of 13 models. Medicine & Science in Sport & Exercise, 2004, 36 (2), 331-335.
- Schutz Y., Weinsier R.L., Hunter G.R. Assessment of free-living physical activity in humans: An overview of currently available and proposed new measures. Obesity Research, 2001, 9 (6), 368-379.
- Shephard R.J. How much physical activity is needed for good health? “Int. J. Sports Med.”, 1999, 20, 23-27.
- Shephard R.J. Limits to the measurement of habitual physical activity by questionnaires. British Journal of Sports Medicine, 2003, 37 (3), 197-206.
- Stasiołek D., Jegier A. Wybrane kwestionariusze stosowane do oceny aktywności ruchowej w różnych grupach wiekowych. Medicina Sportiva, 2003, 37 (11), 563-571.
- Strugarek J. Nowe możliwości obiektywnego pomiaru podstawowych parametrów aktywności fizycznej. Antropomotoryka, 2007, 38, 81-86.
- Szeklicki R. Metody pomiaru aktywności fizycznej. Wychowanie Fizyczne i Sport, 2000, 3, 3-20.
- Vuillemin A., Oppert J.M., Guillemin F. et. al. Self-administered questionnaire compared with interview to assess past-year physical activity. Medicine & Science in Sports & Exercise, 2000, 32 (6), 1119-1124.
- Wilmore J.H., Costill D.L. Physiology of sport and exercise. Human Kinetics Publishers, Champaign, 1999.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE