Integral Estimation of Functional Status of External Respiratory System of Qualified Futsal Players
Фотографии:

ˑ:
V.P. Guba, professor, Dr.Hab., Honorary Figure of Russian Higher Education
Smolensk state university, Smolensk
S.L. Skorovich, Ph.D., senior coach of the Russian national futsal team
Russian Futsal Club. Moscow
V.V. Marinich, associate professor, Ph.D.
Polessky state university, Pinsk, Republic of Belarus
Key words: futsal, functional status, external respiratory system, elite athletes.
Relevance. In the modern conditions of intensification of loads in sports activity new scientific criteria should be developed to estimate the functional state of the respiratory system of qualified athletes [2, 4, 5]. An athlete’s body influenced by permanent loads is characterized by specific conditions that are extremely rare for an average person. Elite futsal players usually cope well with acute and chronic fatigue, overtraining due to excessive physical loading [1, 3].
Increased and extreme physical loading in sport limit physical activity due to the development of bronchial obstruction, cellular infiltration of the bronchial mucosa, remodeling of the respiratory tract. Depending on the loading volume the capacity of the vascular capillary bed increases, along with blood viscosity, extended mucociliary clearance time, while increased pulmonary engorgement at maximum loading in qualified athletes results in compression of the vessels of the pulmonary circuit and development of acute respiratory distress syndrome. It serves as a basis for the respiratory tract remodeling: respiratory muscle hypertrophy occurs, subendothelial fibrosis is being developed, the decrease in elasticity of the bronchial wall is marked, along with ruptures of alveoli and pulmonary capillary occlusion under mechanical and oxidative stress, increased tone of the sympathetic ANS, which leads to vasoconstriction and reduction of the vascular bed.
Recently, researchers have been more interested in such a significant biomarker of immune inflammation as nitric oxide (II) (NO). The concentration of nitrogen oxide in the exhaled air (NOex) increases significantly especially in the case of eosinophilic airway inflammation. However, despite the extensive experience of using this marker, some aspects are still interpreted ambiguously. The relevance of measuring of the athletes’ NOex level is little studied [6-9].
So it is vital to define the clinical relevance of the NOex level in qualified athletes under strenuous loading to estimate the comparability of this marker with bronchospasm manifestations of physical loading, as well as predict bronchial hyperresponsiveness.
The purpose of the present study was to analyze index changes of the flow-volume curve during training of elite futsal players.
Materials and methods. The study involved 26 members of the Russian national futsal team (youth and first team, 2012) aged 18-29 years. The study was performed 4 times: in the morning on an empty stomach, after a workout (in the aerobic mode), after training (during submaximal anaerobic exercise), in the early recovery period using a portable electrochemical NO-analyzer (“NObreath”, Bedfont Scientific Ltd.).
To assess changes in the status of external respiratory function a spirogram was recorded using the spirograph "Spiro Spectrum" by Neurosoft. The spirogram was used to estimate the following indicators: vital capacity (VC), forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), FEV1 / FVC ratio), average air flow rate in the middle of the forced expiration between 25 and 75 % FVC ( SOS 25-75), peak flow rate (PFR), instant expiratory flow rate 25 % FVC (MEF25), instant expiratory flow rate 50 % FVC ( MEFR50 ), instant expiratory flow rate 75 % FVC (MEF75).
Results and discussion. Proceeding from the spirographic monitoring of athletes, the majority of the examined in the analysis of the flow-volume curve had an increase of velocity and volume respiratory indices, which can be described as adequate adaptive responses of the respiratory system, particularly lung ventilation, to the training load (Fig. 1).
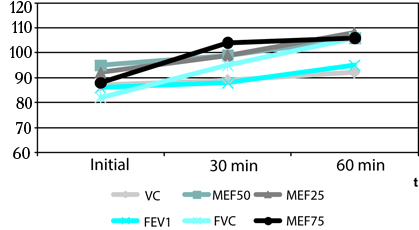
Fig. 1. Indices of external respiratory function in qualified futsal players in dynamics of physical loading.
With the increase in intensity of physical loading during exercise there was a rise in the indicators of respiratory spare abilities (FEV1, FVC, MEF50-75) and of mobilization readiness of the respiratory system to perform additional loading (Fig. 2). These changes were due to involvement of bronchial tubes and bronchioles of the distal respiratory system. The detected capacities indicate the presence of the backup resource of the respiratory system in a group of examined athletes.
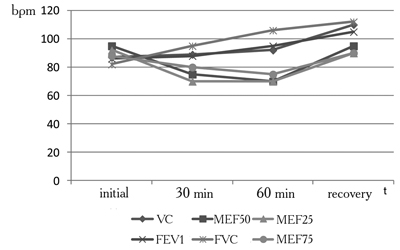
Fig. 2. Indices of external respiratory function in qualified futsal players at build-up of intensity of physical loading
High tolerance of endurance exercises in the studied group of athletes, the chance of growth of fitness and sports skills is expected.
However, some athletes (12%) noted the emergence of maladaptive changes with the increase in training loading up to submaximal level.
The findings prove the reduction of the flow-volume curve indices, characterizing speed capabilities of the respiratory system.
According to the analysis of the results, the deterioration in the external respiratory function is mainly caused by bronchial obstruction due to dysregulation of the autonomic tone with the activation of the parasympathetic division of the autonomic nervous system, reflex decrease of bronchial obstruction in response to lower levels of surfactant in the alveoli, which are observed as a consequence of hypoxic activation of lipid peroxidation processes in response to submaximal loading.
The mean level of NOex was 14,2±0,7 ppb at rest, 21,2±0,4 - after a warm-up, 13,4±0,6 - at build-up of intensity of physical loading, 15,7±0,5 - in the recovery period (Fig. 3).
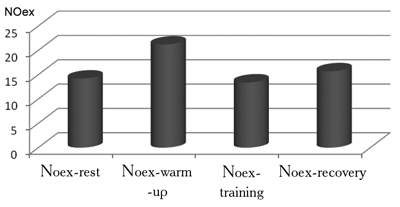
Fig. 3. Expiratory nitrogen oxide in qualified futsal players in various modes of physical loading.
Note. Significance of differences at p<0,05
A significant increase in NO production is marked at build-up of physical loading and preserved overproduction of nitric oxide with exhaled air – during recovery.
This dynamics show the fluctuation in NOex in the area of pathological values, probably associated with a possible immune inflammation. The estimation of FER in the examined athletes has not revealed diagnostically significant decrease in FEV1 MEF25 -75 in dynamics of physical loading.
Conclusion. The changes detected in elite futsal players indicate the need to reduce the intensity of cyclic and speed-strength loading of submaximal power during a training process.
The conducted one-time screening of the dynamics of changes in the concentration of nitric oxide in the exhaled air with the increase in the intensity of physical loading in the youth team has detected the undulating dynamics of NO products, significantly associated with the intensity of anaerobic work. The increase of the NO values above 20 ppb for individual athletes indicates a possible risk of overproduction of this biomarker along with subclinical process of immune inflammation in the respiratory tract. The lack of significant decrease in FEV1 in the examined athletes testifies to sufficient compensatory changes and high respiratory potential of athletes who train speed and strength and endurance abilities. Athletes with average and high production of nitric oxide should be regarded as a group of high risk of bronchial hyperresponsiveness with constant monitoring not only in the national team, but in their club too.
As preventive measures it is desirable to strengthen protein and vitamin and mineral components in the diet, use antihypoxants (succinic acid, coenzyme Q10, mildronat, cytochrome C) during specialized training and in the competition period, regulators of lipid metabolism in the pre-seaon (L-carnitine, lipoic acid), antioxidants in the competition period (vitamins A, C, E, B5, B- carotene). The in-depth phased medical supervision is recommended (once every 3 months).
The monitoring of the indicators of external respiratory function has shown mixed reactions of bronchial tubes of the respiratory tract, autonomic nervous system, local cellular and humoral factors.
The orientation of the processes to adaptation and increase of the oxygen transport function at submaximal loading undergoes reverse development in 15 % of patients that can lead to the realization of the limiting effect of bronchospasm, edema and mucus hypersecretion in response to oxygen supply to the alveoli, and, in turn, provoke a decrease of physical working capacity.
Dynamic monitoring of the training process in the evaluation of the flow-volume curve indices enables (especially in youth team players) to identify at an early phase and correct bronchospasm, caused by physical loading, to clarify its etiology and hold early diagnostic and pharmacological interventions to enhance the effectiveness of the training and competitive processes.
References
- Aliev, E.G. Futsal: textbook for university students in the area of “Physical culture” and the speciality “Physical culture and sport” / E.G. Aliev, S.N. Andreev, V.P. Guba. – Moscow: Sovetsky sport, 2012. – 549 P. (In Russian)
- Guba, V.P. Integral training of football players / V.P. Guba, A.V. Leksakov, A.V. Antipov. – Moscow: Sovetsky sport, 2010. – 208 P. (In Russian)
- Guba, V.P. The basics of sports training: methods of assessment and forecasting (morphobiomechanical approach) / V.P. Guba. – Moscow: Sovetsky sport, 2012. – 384 P. (In Russian)
- Guba, V.P. Integral basics of sports training (methods of assessment and forecasting) / V.P. Guba // LAP LAMBEDT, Academic Publishing. – 2012. – 360 P. (In Russian)
- Zelenin, K.N. Nitric oxide (II): new capabilities of the well known molecule / K.N. Zelenin // Sorosovskiy obrazovatel’ny zhurnal. – 1997. – № 10. – P.105-110, 852-857. (In Russian)
- Tsyplenkova, S.E. Exhaled nitric oxide: diagnostic capabilities of pediatric pulmonology: / S.E. Tsyplenkova, Yu.L. Mizernitsky // Tikhookeanskiy meditsinskiy zhurnal. – 2006. – № 4. – P. 149-150. (In Russian)
- Leone, A., Gustafsson, L., Francis, P., Persson, M., Wiklund, N., Moncada, S. Nitric oxide is present in exhaled breath in humans: direct GC-MS confirmation. // Biochem Biophys Res Commun 1994; 201: 883-887.
- Alving, K., Weitzberg, E., Lundberg, J. Increased amount of nitric oxide in exhaled air of asthmatics. //Eur Respir J 1993; 6:1368-1370.
- Barnes, P., Kharitonov, S. Exhaled nitric oxide: a new lung function test. //Thorax, 1996; 51: 233-237.
Author's contacts: reasm2008@mail.ru


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE