High-altitude hr variability rating tests in extreme mountaineering sport
ˑ:
Dr.Hab., Associate Professor S.N. Litvinenko1
Dr.Hab., Professor Y.V. Baykovsky1
Associate Professor, PhD N.S. Shumova1
Master's student A.A. Mitrofanov1
1Russian State University of Physical Education, Sports, Youth and Tourism (SCOLIPE), Moscow
Keywords: daily ECG profiles, heart rate variability, spectral amplitudes, extreme conditions, sympathetic and parasympathetic system effects.
Introduction. Modern extreme high-altitude mountaineering sport is associated with multiple risk factors for cardiac functions as verified by the cardio-intervals and spectral amplitudes of the cardio-intervalograms [2]; albeit the heart rate (HR) variability appears to be still underexplored. Among these risk factors are: early awakening; continuous (up to 12-16 hrs) physical loads of high intensity; integrated effects of high altitude conditions, in particular altitude and associated hypoxia; weather conditions (wind, frost); difficulty moving over snowy and icy terrain; sense of danger in the event of possible fall [1, 3].
Objective of the study was to profile the ECG rates in the extreme mountaineering process.
Methods and structure of the study. The study was designed to obtain the daily ECG profiles in 2 volunteer mountaineers (31 year-old males having no sports category and climbing Elbrus for the first time) in ascendancy on the Elbrus (5,642m high) peak using the hardware-software complex "Valenta-MN-02-8.1" (LLC "Neo Company", St. Petersburg). The electrodes were placed in the tent on the 4,380m altitude at 7-8 p.m., then the subjects fell asleep, woke up in the morning, performed their high-altitude climbing, climbed down, after which the ECG recording was stopped.
Taken for analyses were the 8-12min ECG artifact-free segments averaged with account of the following: SLEEP period on the 4,380m altitude from 9 p.m. to 1:50 a.m. (waking up to an alarm clock); WORK period, i.e. ascendance from the 4,380m point to the 5,642m peak taking around 9 hours; REST time including the 10+ min rest breaks; PEAK time, i.e. stay on the Elbrus peak; DESCENT time to reach the tents for 3-4 hours; and the FINISH time, i.e. rest in the tents upon the descent.
Results and discussion. The statistical indicators of cardio-intervalograms averaged with account of the subjects’ states are presented in the table.
Statistical indicators of distribution of R-R intervals
|
States |
HR (bpm) |
Mode (Мо, ms) |
Mode amplitude (АМо, %) |
Average duration (ms) |
MSD (ms) |
Coefficient of variation (CV, %) |
|
SLEEP |
71 |
822 |
9.5 |
849 |
56.6 |
6.4 |
|
WORK |
142 |
413 |
42.6 |
418 |
9.4 |
2.2 |
|
REST |
116 |
501 |
14.4 |
517 |
39.8 |
7.7 |
|
PEAK |
115 |
496 |
15.0 |
520 |
43.6 |
8.4 |
|
DESCENT |
136 |
435 |
29.4 |
436 |
13.3 |
3.0 |
|
FINISH |
100 |
588 |
12.2 |
606 |
35.0 |
5.8 |
The mean heart rate and heart rate variability indices in different states are presented in Fig. 1.
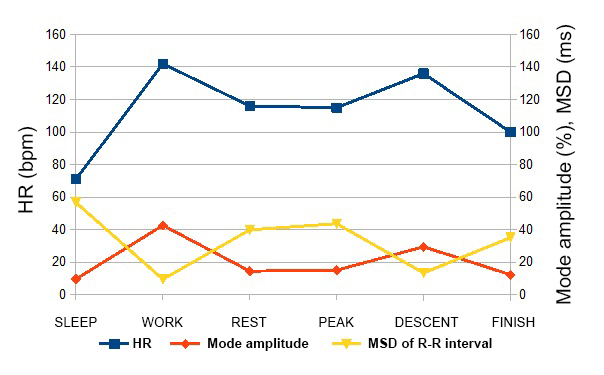
Fig. 1. HR indices, mean square deviations (MSD) and mode amplitudes in different states
As seen from Fig. 1, the HR indices and mode amplitudes change unidirectionally, while the standard deviation indices are in reverse phase. Thus, during the transition from sleep to active wakefulness and intense muscular activity, HR increases twofold; moreover, the HR variability decreases significantly, and the mode amplitude increases. During rest and upon reaching the peak, these indicators decrease, then they increase again during the descent.
The spectral characteristics of cardio-intervalogram in different states are presented in Fig. 2 and 3.
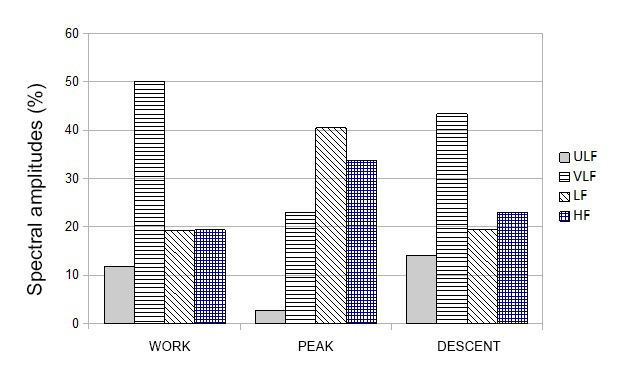
Fig. 2. WORK-PEAK-DESCENT spectral amplitudes
As seen from Fig. 2, the states associated with intense muscular activity are characterized by the significant dominance of the VLF waves. The spectral amplitudes of these waves reach 50% during WORK and 43% during the DESCENT. These waves are associated with the activity of the central ergotropic and humoral-metabolic mechanisms, i.e. directly correlate with the processes of energy supply of intense cardiac activity [2].
The spectral analysis of the states SLEEP – REST – FINISH (see Fig. 3) shows that it is the slow modes of the LF range with the period of 10–30 sec, associated with sympathicotonic effects of the medulla oblongata from the vasoconstrictor and cardiokinetic centers, that dominate in these states. At the same time, during SLEEP it is the HF waves with the period of 2.5-6.5 sec, directly associated with the respiratory movements and vagotonic effects, that become predominant in the spectrum.
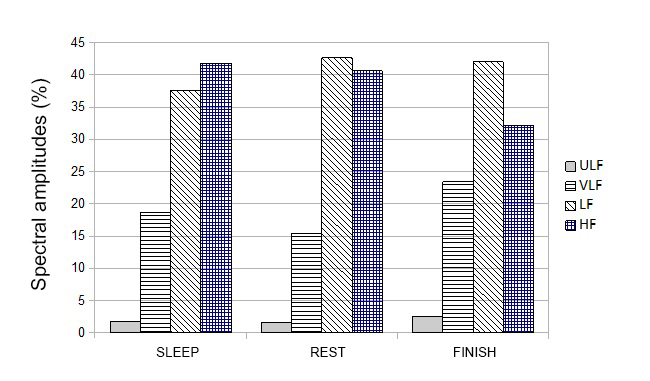
Fig. 3. SLEEP-REST-FINISH spectral amplitudes
The comparative analysis of spectral characteristics of such resting states as SLEEP, REST, FINISH and PEAK, reveals that at the Elbrus peak there is also an increase of the LF and HF waves, despite the stress impact of considerable hypoxia, fatigue, strong wind, and frost. However, during the DESCENT, these waves get suppressed, and the VLF waves associated with the ergotropic influences start dominating again thus providing the activity of the muscle groups involved.
The spectral indices characterizing the general trends in the sympathetic and parasympathetic system effects in different states are presented in Fig. 4.
The obtained data on the correlation between the spectral amplitudes within different ranges show that the LF/ HF indices slightly change in different states, despite the variations in the absolute values. At the same time, the VLF/ HF indices and IC=(VLF+LF)/HF indices change in a high-degree synchronicity, which can apparently be explained by a significant increase in the absolute values of the LF and VLF spectral amplitudes.
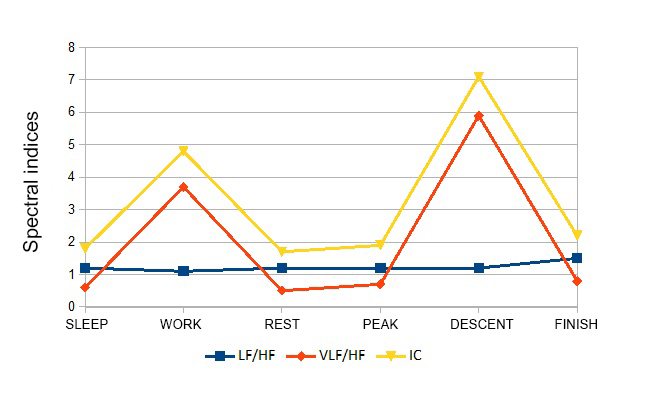
Fig. 4. Spectral indices in different states
Interestingly, the greatest increase in these indices was registered during the DESCENT, although the maximum absolute power of VLF waves was observed during WORK.
Conclusions. The statistical and spectral characteristics of cardio-intervalogram at different stages of high-altitude mountaineering testify to the increase of both sympathetic and parasympathetic system effects on the HR variability data.
References
- Baykovskiy Y.V., Baykovskaya T.V. Faktoryi, opredelyayushchie trenirovku sportsmena v usloviyakh vysokogorya i srednegorya [Factors to determine athlete's training in high and middle altitudes]. Moscow: Divizion publ., 2010, 280 p.
- Kovaleva A.V., Panova E.N., Gorbacheva A.K. Analiz variabelnosti ritma serdtsa i vozmozhnosti ego primeneniya v psikhologii i psikhofiziologii [Analysis of heart rate variability and its potential for use in psychology and psychophysiology]. Sovremennaya zarubezhnaya psikhologiya, 2013, no. 1, pp 35-50.
- Litvinenko S.N., Baykovskiy Y.V. Regulyatsiya serdechnogo ritma v protsesse akklimatizatsii k vysokogornomu voskhozhdeniyu [Heart rate regulation during acclimatization to alpine ascent]. Ekstremalnaya deyatelnost cheloveka, 2018, no. 3 (49), pp. 46-49.
Corresponding author: litvinenko_svetlana@yahoo.com
Abstract
Modern extreme high-altitude mountaineering sport is associated with multiple risk factors for cardiac functions as verified by the cardio-intervals and spectral amplitudes of the cardio-intervalograms; albeit the HR variability appears to be still underexplored. The study was intended to bridge some gaps in the knowledgebase by profiling the ECG rates in the extreme mountaineering process. The study was designed to obtain daily ECG profiles in 2 volunteer 31 year-old male mountaineers in ascendancy on Elbrus (5642m high) peak. Taken for analyses were the 8-12min ECG segments averaged with account of the following: SLEEP period on the 4380m altitude starting from 9 p.m. to 1:50 a.m.; WORK period i.e. ascendance from the 4380m point to 5642m peak, taking 9 hours; REST time including the 10+min rest breaks; PEAK time i.e. stay on the Elbrus peak; DESCENT time to reach the tents for 3-4 hours; and the FINISH time, i.e. rest in the tents upon the descent. Analyses of the statistical data and ECG data show the increased sympathetic and parasympathetic system effects on the HR variability data in the extreme mountaineering process.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE