Tuvan junior males' heart rhythm control specifics under variable physical loads
Фотографии:

ˑ:
PhD, Associate Professor S.K. Saryg1
Postgraduate A.D. Lopsan1
Dr.Biol., Professor L.K. Buduk-ool1
1Tuvan state university, Kyzyl
The relevance of the problem of adaptation of Tuvan junior males involved in the training process of different orientations is due to the effects on their body of not merely high education and training workloads, but also uncomfortable natural and climatic conditions. Athletes’ awareness of the peculiarities of adaptation shifts resulting from structural, physiological and biochemical changes plays a key role in choosing the correct training process to develop certain qualities, which also determines the practical significance of the study.
Objective of the study was to analyze the peculiarities of heart rate variability and adaptive reserves of the body of Tuvan junior males with different levels of motor activity under the influence of physical loads.
Methods and structure of the study. The study involved 41 volleyball players (V) and 40 rated freestyle wrestlers (W) of the Olympic Reserve School; 43 junior males engaged in body conditioning (BC) studying in Kyzyl State Pedagogical Institute; 40 male students of the architectural college (Reference Group - RG). Mean age - 18.7±0.1 y.o.
HRV was studied based on the results of cardiointervalogram recorded using the hardware-software complex "Poly-Spectrum-12" (by "NeuroSoft" Ltd., Ivanovo, Russia). First, HRV was recorded in a sitting position (background), then the students were tested on the "Proteus RES-7097" cycle-ergometer (Germany) with an increasing load - from 50 to 100 W, with 5-min pauses, between which their heart rhythm was recorded. The duration of each load test was 5 minutes. The following HRV parameters were used during the analysis: SDNN, ms (total RR interval variability index throughout the period under study), RMSSD, ms (activity of the parasympathetic unit of autonomous regulation), pNN50,% (percentage of successive NN intervals differing by more than 50 ms throughout the period under study), TP, ms2 (spectrum total power), VLF, ms2 (very low-frequency oscillations), LF, ms2 (low-frequency oscillations) and HF, ms2 (high-frequency oscillations). We also measured the following parameters: LF/ HF (autonomic balance), TI, c.u. (regulatory systems tension index), CI, c.u. (centralization index) [CI = (VLF+LF)/HF] as an integral indicator reflecting the dominance of the central and sympathetic influences on the autonomous contour of regulation of the heart functions. HRV was evaluated according to the International Standard proposed by the North American Society of Pacing and Electrophysiology and European Society of Cardiology [10]. The results obtained were statistically processed using the Statistica 6.0 software. We calculated the arithmetic mean (M) and standard error (m). The significance of differences in absolute values was determined by the parametric Student's t-test (used to estimate independent, normally distributed samples). The differences between the values at the level of p≤0.05 were deemed statistically significant. All subjects were informed on the nature and purpose of the study and gave their written consent to participate in it.
Results and discussion. The distribution of the young males by the HRV types revealed some significant differences between the groups (see Figure 1).
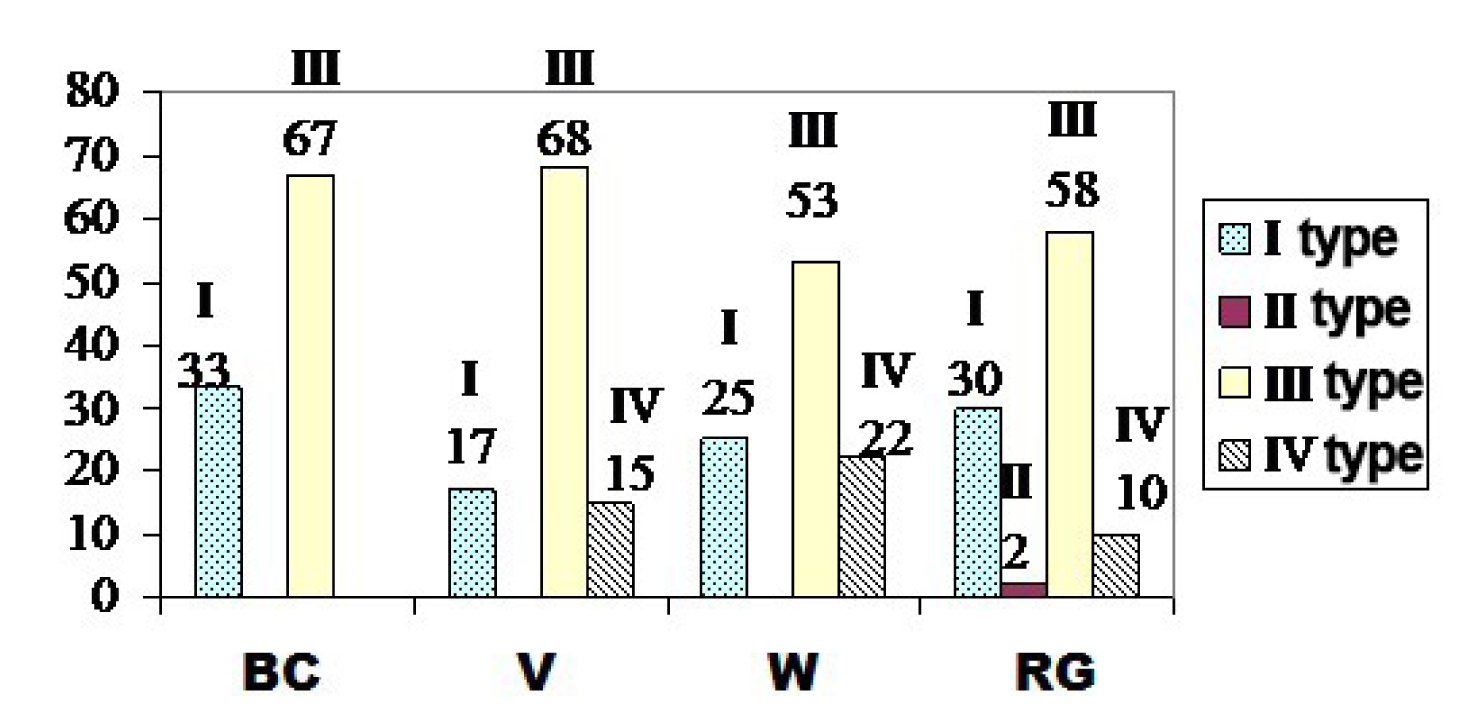
Figure 1. Distribution of junior males with different levels of motor activity by heart rhythm autonomic response types (according to HRV analysis), %
We found the I/ III autonomic control types to prevail in all groups. ACT I is characterized by moderate predominance of the central regulation of heart rhythm, decreased activity of the autonomous contour and, in general, moderate tension of the regulatory systems; ACT III - by moderate predominance of the heart rhythm autonomic regulation, which makes it possible to characterize the functional state of the regulatory systems as optimal [7].
Subsequently, we analyzed only the values obtained in the ACT I/ III juniors, since these types were found in all groups.
The obtained baseline values of HRV (at rest) (Table 1, 2) were compared with those obtained after different physical loads (50 W and 100 W).
Indicators |
SDNN, ms |
RMSSD, ms |
pNN50, % |
|||
ACT I |
ACT III |
ACT I |
ACT III |
ACT I |
ACT III |
|
BC |
||||||
Baseline 50 W 100 W |
38.5±1.4 39.5±2.2 44.6±2.6 |
55.1±2.0#* 56.7±2.6#* 62.8±3.6 |
22.2±1.6 22.0±1.9 20.5±3.0 |
39.5±2.4* 39.3±2.7#○ 36.4±5.5 |
4.0±1.0 2.8±0.6 1.7±0.6 |
19.0±2.4*2 18.4±2.23 11.3±1.9 |
V |
||||||
Baseline 50 W 100 W |
38.4±3.8 48.2±6.0 40.4± 3.6 |
58.0±2.2&^ 58.0±2.5& 65.2±3.4 |
25.5±5.0 35.0±8.5 22.7±2.3 |
45.0±2.8^ 41.9±3.0 41.3±4.1 |
7.6±4.9 5.6±1.4 3.7±1.9 |
21.4±2.7 20.2±2.7 16.2±2.6 |
W |
||||||
Baseline 50 W 100 W |
36.6±2.2 39.6±2.9 45.9±4.5 |
66.0±3.01 77.4±4.5 68.3±4.3 |
23.2±2.4 26.3±3.8 24.4±4.6 |
45.4±3.3 54.6±7.2 47.7±4.5 |
5.2±2.2 7.5±3.2 3.7±1.8 |
19.8±2.9 19.2±2.8 16.3±2.7 |
RG |
||||||
Baseline 50 W 100 W |
39.0±2.1 41.2±3.3 39.2±2.7 |
68.1±3.5 66.2±3.5 68.0±4.6 |
24.8±1.7 29.4±6.0 17.3±4.8 |
58.5±5.72 51.3±4.4 39.9±5.3 |
4.8±1.0 9.2±4.4 6.5±3.8 |
30.7±4.52 25.4±3.73 12.6±3.2 |
Note. Here and in Table 2: changes are statistically significant (р≤0.05) in relation to: ○ – BC and V groups; # − BC and W groups; * – BC and Reference groups; & − V and W groups; ^ − V and Reference groups; + − W and Reference groups; 1 – baseline and 50 W load; 2 – baseline and 100 W load; 3 − 50 и 100 W loads.
Indicators |
ТР, ms2 |
VLF, ms2 |
LF, ms2 |
HF, ms2 |
|||||
ACT I |
ACT III |
ACT I |
ACT III |
ACT I |
ACT III |
ACT I |
ACT III |
||
BC |
Baseline |
2017.3± 149.52 |
3713.0± 271.7#*2 |
936.6± 120.52 |
1462.3± 150.9#*12 |
790.5± 90.8 |
1630.2± 185.2 |
275.4± 35.3 |
719.0± 78.3* |
50 W |
2131.2± 205.13 |
4194.8±297.4# |
1081.5± 150.73 |
1931.9± 171.9#3 |
788.5± 66.1○ |
1543.1± 173.6# |
261.0± 48.4 |
754.0± 78.8* |
|
100 W |
3052.0±388.8 |
5541.6± 627.0 |
1993.0± 395.5 |
3100.3±297.3 |
800.8±99.6* |
1478.6±194.1 |
257.8±56.8 |
962.8± 366.6 |
|
V |
Baseline |
2034.4± 324.3 |
4054.1± 339.4^2 |
785.7± 185.3 |
1432.3± 155.8&^2 |
965.7± 150.0 |
1741.7± 241.9 |
283.0± 43.9 |
880.0± 126.0 |
50 W |
3181.7 ±657.4 |
4160.5± 360.4&3 |
1139.7 ±396.8 |
1834.7± 167.8&3 |
1544.5± 281.0^&3 |
1540.2± 187.5& |
497.5± 152.5 |
785.5± 130.1 |
|
100 W |
2528.4± 397.9 |
5795.5± 704.2 |
1366.8±408.1 |
3603.3± 598.7 |
884.0±107.1^ |
1455.8±195.0 |
277.6±71.1 |
736.2± 125.0 |
|
W |
Baseline |
1852.1± 219.92 |
5145.9± 435.31 |
891.1± 185.82 |
2100.4± 245.41 |
707.4± 76.3 |
2246.3± 257.4 |
253.5± 34.4 |
799.0± 114.9 |
50 W |
2104.9± 263.4 |
7123.3± 645.1+ |
940.0± 202.63 |
3192.5±381.7 |
898.5±97.6 |
2599.5± 181.5+3 |
267.0± 47.8 |
1331.5± 358.5 |
|
100 W |
3332.9± 580.7 |
6058.9± 687.5 |
2427.0±470.2 |
3137.4±498.5 |
679.1±98.1+ |
1969.5±161.6 |
226.9± 47.3 |
951.8± 147.8 |
|
RG |
Baseline |
2093.0± 309.6 |
5240.4± 495.9 |
983.7± 185.32 |
2346.0± 296.12 |
813.0± 207.3 |
1537.2±99.5 |
296.3± 30.9 |
1369.7± 264.8 |
50 W |
2323.2± 263.6 |
5268.3± 526.5 |
1083.8 ±187.5 |
2411.0±273.93 |
690.7±113.83 |
1695.5±192.0 |
548.8±201.8 |
1161.0± 191.3 |
|
100 W |
2660.3± 426.6 |
6730.6± 892.7 |
2034.3±435.4 |
4289.7±635.2 |
402.3±67.2 |
1575.0±239.7 |
223.9±89.7 |
866.1± 191.0 |
|
In the initial state (background) the ACT III RG had higher values of TP and VLF as compared to the BC and V groups, which indicated increased neurohumoral effects on the heart rhythm due to a larger VLF-component. Physiological interpretation of the VLF-waves is ambiguous. It was found that the level of VLF-oscillations depends on the nature of oxygen consumption; in some cases the VLF-component comprises mainly humoral-metabolic influences [4]. Increasing VLF-component, probably, testified to the mobilization of metabolic and energy reserves of the body under the influence of functional stress and a hyperadaptive reaction [5]. After increased physical load (100 W) the LF-component was found to be lower in the RG than in the BC, V and W groups, which indicated lower activity of the sympathetic regulation unit in the RG as opposed to the latter. The ACT III volleyball players demonstrated high VLF values in the initial state compared with the W group, after 50 W load - a significant increase in TP, VLF and LF - increased activity of the central regulation contour. After physical load of 50 W, the BC and W groups were found to have increased activity of the adaptation mechanisms. The VLF-component (VLF˃LF˃HF) increased in the V group, and after increased physical load (100 W), a hyperadaptive reaction to stress was observed. In the V and W groups, the LF-component decreased significantly after physical load (50 W), thus indicating inactivation of the central contour.
In the resting state (background) in the BC and W groups the SDNN and RMSSD values were within the normal limits, pNN50 - slightly below the norm; in the V group the time indices were within the normal limits; in the RG the SDNN value was within the normal range, and RMSSD and pNN50 values - above the norm. In the initial state, the LF˃VLF˃HF spectrum type changed to VLF˃LF˃HF after physical load (50 W) in all groups, which was probably due to the mobilization of metabolic and energy reserves under the influence of functional stress, which led to a hyperadaptive state. A significant decrease in the pNN50 value in the BC group testified to the increase of sympathetic regulation after increased physical load (100 W). In the RG - a significant decrease in the pNN50 and RMSSD values, increased TI after increased load (100 W) (from 52.0±5.4 to 77.2±11.2), which indicated increased activity of the central regulation contour and overtension of the regulatory systems. In the V group, a significant increase in SDNN after exercise (50 W) testified to an increase in the autonomic regulation. After exercise, the BC, V (100 W) and W (50 W) groups were found to have an increase in the TP value due to an increase of the VLF-component. In the RG, the very low-frequency component of the spectrum increased significantly without any significant increase in TP, which indicated a hyperadaptive reaction. The centralization index (CI) increased significantly in the groups of ACT III BC and V, a sharp increase was also observed in the ACT I/ III RG after increased physical load (100 W).
Conclusions. The study sample was dominated by the junior males classified with Autonomic Control Types (ACT) I and III. The regulatory system response to physical loads depended on the initial type of autonomic regulation. The ACT I junior males were tested with generally lower variations in the cardiovascular system test rates versus the ACT II juniors. The high physical loads were responded by the physically active young males by the autonomous control strengthening and growing activity of the central control contour with the further growth of the load. At the same time, physically inactive junior males responded to the loads (regardless of the load factor), by the growing activity of the central control contour that may be interpreted as the unspecific component of the adaptive response to different stressors. The ACT I/ III junior males engaged in body conditioning practices, ACT III volleyball players and ACT I/ III wrestlers were tested with fairly high HR variability. The ACT I junior males involved in body conditioning practices and wrestling were tested with the increased adaptive capabilities (the adaptation reserve had formed); and the volleyball players and physically inactive juniors were tested with the optimal functionality level (the adaptive abilities being within the conditional norm). The ACT III body conditioning group, volleyball and wrestling groups were tested with notably increased adaptation capabilities; and the physically inactive junior group was tested with an autonomic imbalance as a result of high physical loads (autonomic imbalance had been eliminated).
References
- Aghajanyan N.A., Batotsyrenova T.E., Severin A.E. et al. Sravnitelnye osobennosti variabelnosti serdechnogo ritma u studentov, prozhivayuschikh v razlichnykh prirodno-klimaticheskikh regionakh [Comparative features of heart rate variability in students living in different natural and climatic regions]. Fiziologiya cheloveka, 2007, no. 33 (6), pp. 66-70.
- Mikhaylov V.M. Variabelnost serdechnogo ritma: opyt prakticheskogo primeneniya metoda [Heart rate variability: experience of practical application of the method]. Ivanovo: Ivanovo state medical academy publ., 2002, 290 p.
- Fomin L.M. Borba «Khuresh» kak sredstvo vospitaniya volevykh kachestv studentov: Tezisy region. nauch.-prakt. konf. [Khuresh wrestling to develop strong will in students. Proc. region. res.-practical conf.]. Kyzyl, 1989, 56 p.
- Chuyan E.N., Biryukova E.A., Ravaeva M.Y. Fiziologicheskie mehanizmy variabelnosti serdechnogo ritma (obzor literatury) [Physiological mechanisms of heart rate variability (literature review)]. Uchenye zapiski Tavricheskogo nats. un-ta im. V.I. Vernadskogo. Ser.: Biologiya, khimiya, 2008, vol. 21 (60), no. 3, pp. 168-189.
- }Shlyik N.I. Serdechny ritm i tip regulyatsii u detey, podrostkov i sportsmenov [Heart rate and type of regulation in children, adolescents and athletes]. Izhevsk: UU publ., 2009, 255 p.
- Task Force of the European of Cardiology and the North American Society of Pacing and Electrophysiology. Heart Rate Variability. Standards of Measurement, Physiological Interpretation, and Clinical Use. Circulation. 1996; 93: 1043-1065.
Corresponding author: s.k.sailyk@mail.ru
The study analyses the Tuvan junior males’ (17-21 year-old) heart rate variability data versus varied physical loads. High education and training loads were profiled versus the environmental, anthropometrical, psychic, physiological and ethnic factors and specifics that give the reasons to consider the study innovative. The study sample was dominated by the junior males classified with Autonomic Control Types (ACT) I and III. The ACT I junior males were tested with generally lower variations in the cardiovascular system test rates versus the ACT II juniors. The sample responded to high physical loads with the autonomous control strengthening and growing activity of the central control contour with the further growth of the load. Physically inactive junior group responded to the loads (regardless of the load factor), by the growing activity of the central control contour that may be interpreted as the unspecific component of the adaptive response to different stressors. The ACT I/ II junior males engaged in body conditioning practices, ACT III volleyball players and ACT I/ III wrestlers were tested with fairly high HR variability. The body conditioning junior group and ACT I wrestling group was tested with the increased adaptive abilities; and the volleyball players and physically inactive juniors were tested with the HR variability within the conditional norm. The body conditioning group, volleyball group and ACT III wrestling group were tested with notably increased adaptation abilities; and the physically inactive junior group was tested with an autonomic imbalance as a result of high physical loads.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE