Medical students' health and physical culture improvement by individualized practices
Фотографии:

ˑ:
D.A. Ulyanov
Volgograd State University, Volgograd
Keywords: Special Medical Department, education process, functional status, physical fitness, somatic health.
Introduction. Our analysis of the Special Medical Department students’ diagnosed disease structure showed that they suffer from a wide variety of cardiovascular, musculoskeletal, respiratory, gastrointestinal, endocrine, nervous, urinogenital, vision system and skin/ subcutaneous cellular tissue diseases. Special work was performed to group the subject students into special groups based on the disease classes – on the assumption that it is the detailed disease profiling analysis that should form a basis for further initiatives to improve the students’ educational efficiency by the relevant physical education tools being prudently selected for every nosological/ disease group of students.
Objective of the study was to find correlations of the functional state, physical fitness and somatic health rates for different health groups of the Special Medical Department students.
Methods and structure of the study. The study data and analyses were used to find correlations of the functional state, physical fitness and somatic health rates in different health groups of the Special Medical Department students. Subject to the study were 194 students of both sexes (academic year 1–4) diagnosed with different health conditions. The study was designed to obtain the following test data: resting heart rate (HR); vital capacity (VC) rates; Stange's test (breath-holding test during inspiration) rates; 100 m sprint; standing jump; 3000/ 2000 m combined (with walking) race times for men/ women, respectively; pull-ups on high/ low horizontal bars for men/ women, respectively; and somatic health rates.
The analysis produced, among other things, the following data: the Group 1 young men (diagnosed with cardiovascular, respiratory and central nervous system diseases) showed 14 significant correlations of the study rates including five 1%-significant correlations; with the most close correlations found for the 100 m sprints times versus the stand jump results (r = - 0.526); resting heart rates versus the 3000 m race times (r = - 0.478); and the vital capacity rates versus the Stange's test rates (r = - 0.472); with every of the analyzed characteristics being rated as systemic.
The attempted distribution of the study rates using the maximal correlation path method made it possible to group them in a chain. Such presentation of the study data, however, gave no way to indentify a central segment and distribution branches of the data array. This fact made it difficult to identify the most important rates of potential highest benefit for the education process and health improvement project. Notwithstanding that, there are fair grounds to give preference to the resting heart rates, 3000 m combined race times, the Stange's test rates and the 100 m sprit times that were found to group around the centre of the study data distribution chain (see Figure 1).
The Group 2 young men (diagnosed with gastrointestinal, endocrine, urinogenital and vision system diseases) showed 16 significant correlations of the study rates including four 1%-significant correlations; with the most close correlations found for the resting heart rates versus the 3000 m combined race times (r = - 0.465); the vital capacity rates versus the 3000 m combined race times (r = - 0.435); and the resting heart rates versus the Stange's test rates (r = - 0.433).
The 3000 m combined race and 100 m sprint times were found to form a trunk segment of the distribution chain, with the following test rates forming the following four branches: vital capacity rate – Branch 1; standing jump result – Branch 2; pull-ups on the bar – Branch 3; and resting heart rate, Stange's test rate and somatic health rate – Branch 4. Our study results were indicative of the run races on the whole and the 3000 m combined (with walking) race in particular being most important for the Group 2 students’ health improvement initiatives.
The Group 3 students (diagnosed with musculoskeletal diseases) showed 14 significant correlations of the study rates including three 1%-significant correlations; with the most close correlations found for the resting heart rates versus the 3000 m combined race times (r = - 0.477); the Stange's test rates versus the somatic health rates (r = - 0.435); and the 100 m sprint time versus the 3000 m combined race times (r = - 0.435).
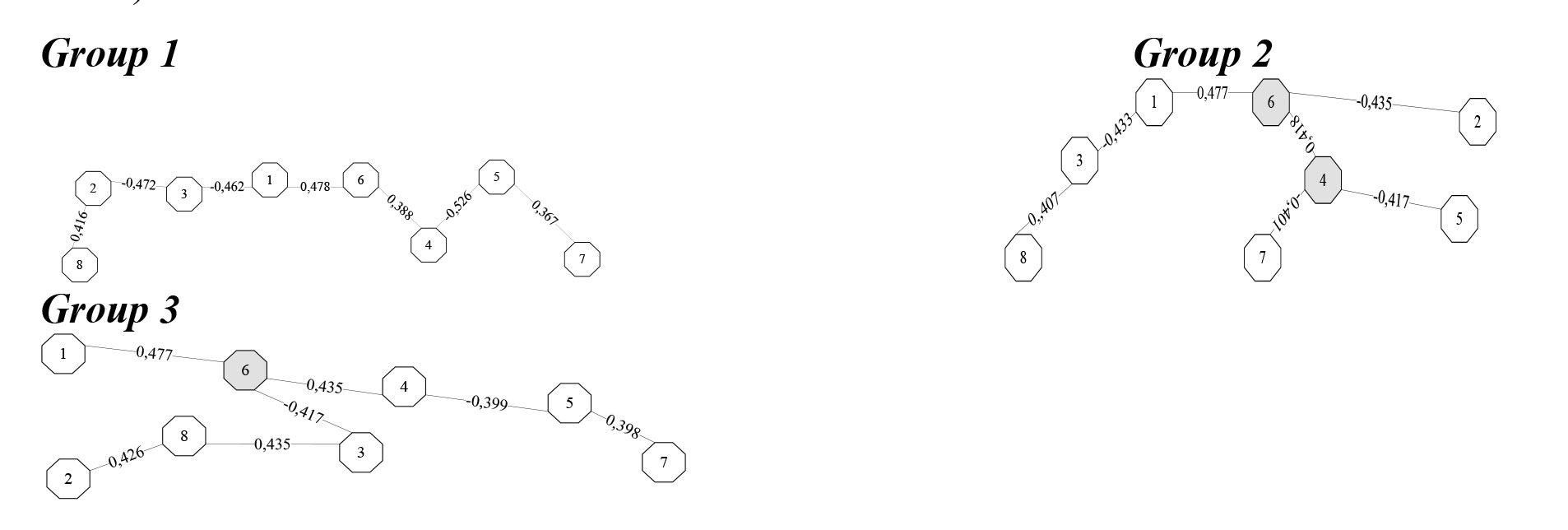
Figure 1. Functional state, physical fitness and somatic health rate correlation dendrograms of the Special Medical Department men’s health groups
Note: 1 – resting heart rate; 2 – vital capacity rate; 3 – Stange's test rate; 4 – 100 m sprint time; 5 – standing jump result; 6 – 3000 m combined (with walking) race time; 7 – pull-ups count; 8 – somatic health rate.
The 3000 m combined (with walking) race was singled out as a trunk part of the distribution chain, with the following three branches (including two integrated ones): resting heart rate – Branch 1; vital capacity rate, Stange's test rate and somatic health rate – Branch 2; 100 m sprint time, stand jump result and pull-ups count – Branch 3. Therefore, the 3000 m combined (with walking) race was rated as a key practice for the Group 3 students’ health improvement initiatives.
The young women’s performance data were also analyzed using the maximal correlation path method. The Group 1 young women showed 14 significant correlations of the study rates including six 1%-significant correlations; with the most close correlations found for the Stange's test rates versus the 3000 m combined race times (r = - 0.509); the vital capacity rates versus the Stange's test rates (r =- 0.485); and the 100 m sprint rates versus the stand jump results (r = - 0.478). The trunk part included the standing jump results and the 3000 m combined race times; with the following four distribution branches: the 100 m sprint rate – Branch 1; pull-ups on the low bar – Branch 2; somatic health rate - Branch 3; resting heart rate, vital capacity rate and Stange's test rate – Branch 4 (see Figure 2). Therefore, the study found one integrated and three multi-component branches for this Group, with the 3000 m combined (with walking) race and standing jump rated as key practices for the Group 1 young women’s health improvement initiatives.
The Group 2 young women showed 13 significant correlations of the study rates including seven 1%-significant correlations; with the most close correlations found for the somatic health rates versus the 3000 m combined (with walking) race time (r = - 0.517); the vital capacity rate versus the Stange's test rate (r = - 0.513); and the 100 m sprint time versus the standing jump result (r = - 0.501).
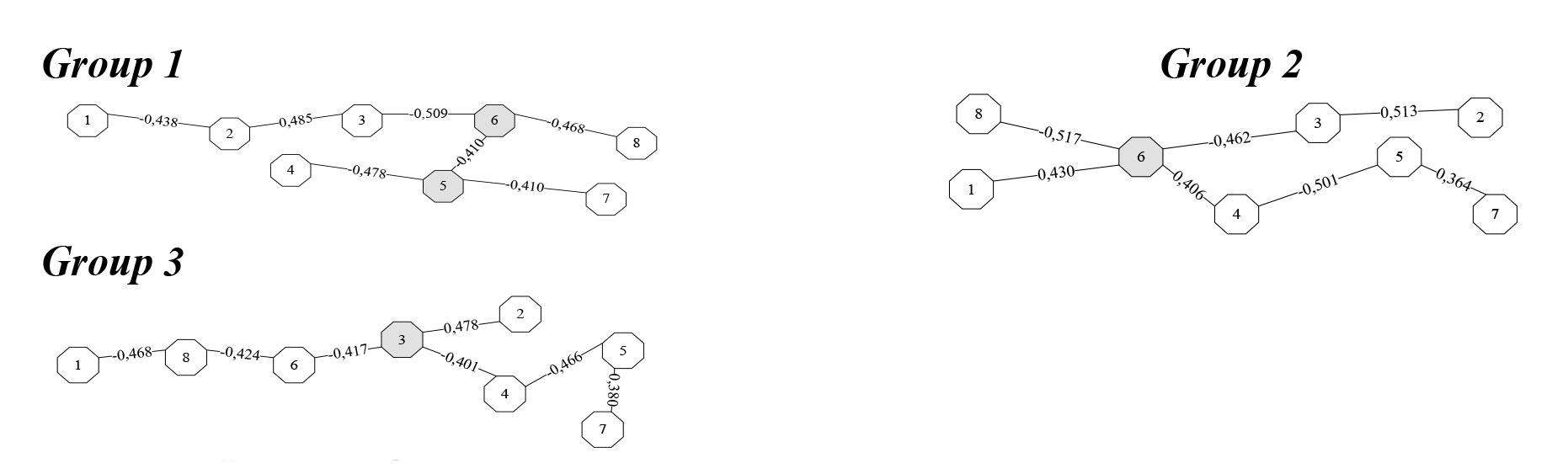
Figure 2. Functional state, physical fitness and somatic health rate correlation dendrograms of the Special Medical Department women’s health groups
Note: 1 – resting heart rate; 2 – vital capacity rate; 3 – Stange's test rate; 4 – 100 m sprint time; 5 – standing jump result; 6 – 3000 m combined (with walking) race time; 7 – pull-ups count; 8 – somatic health rate.
It was the 3000 m combined (with walking) race that formed the central segment of the distribution chain, with the following four branches: somatic health rate – Branch 1; resting heart rate – Branch 2; vital capacity rate and Stange's test rate – Branch 3; and 100 m sprint and pull-ups – Branch 4.
The Group 3 young women’s results were distributed as follows: the Stange's test formed a central segment of the distribution chain, with the following three branches: vital capacity rate – Branch 1; 100 m sprint, standing jump and pull-ups – Branch 2; and resting heart rate, somatic health rate and 3000 m combined race time – Branch 3.
Conclusion. Our study results and analysis identified a few specific correlations in distribution of the functional state, physical fitness and somatic health rates for different health groups of the Special Medical Department students. The data distribution patterns made it possible to individualize the health-improvement tools of the physical education process, select the physical practices best tailored to the individual health conditions and rate the workloads depending of the students’ actual physical fitness rates.
References
- Ulyanov D.A. Vliyanie fizkul'turno-ozdorovitel'noy deyatel'nosti na formirovanie u studentov potrebnosti v zdorovom obraze zhizni (Influence of health and fitness activities on formation of students' healthy lifestyle needs) / D.A. Ulyanov, T.G. Kovalenko, A.P. Shklyarenko // Teoriya i praktika fiz. kultury. – 2013. – № 4. – P. 40-41.
- Ulyanov D.A. Otsenka funktsional'nogo sostoyaniya zdorov'ya molodezhi v obrazovatel'noy srede (Assessment of functional state of health of young people in educational environment) / D.A. Ulyanov, O.V. Fedyakina, A.P. Shklyarenko, T.G. Kovalenko // Fizicheskaya kul'tura: vospitanie, obrazovanie, trenirovka. – 2015. – № 1. – P. 69-71.
- Kovalenko T.G. Theoretical-systems approach to developing health model / T.G. Kovalenko // Book of Abstracts. 10 th Annual ECSS-Congress of the European College of Sport Science (13-16 July, 2005). - Belgrad, Serbia. – 2005. – P. 205-206.
- Kovalenko T., Ulyanov D., Shklyarenko A. INFORMATIVE AND HEALTH-IMPROVING TECHNOLOGIES IN HIGH SCHOOL PHYSICAL EDUCATION OF MEDICALLY FRAGILE STUDENTS // Book of Abstracts. Sport Sciences: Nature, Nurture and Culture: 14th Annual ECSS-Congress of the European College of Sport Science (June 24-27). – Oslo/Norway, 2009. – P. 240.
- Ulyanov D., Kovalenko T., Shklyarenko A. ACTUAL TECHNOLOGIES IN HIGH SCOOL EDUCATION // Book of Abstracts. Sport Sciences: Nature, Nurture and Culture: 14th Annual ECSS-Congress of the European College of Sport Science (June 24-27). – Oslo/Norway, 2009. – P. 449.
Corresponding author: sport@volsu.ru
Abstract
Special emphasis is being made today by the Special Medical Department of the Volgograd State University on the policies to improve the students’ physical education quality and thereby solve a variety of critical issues related to the students’ personal physical culture, health standards, active lifestyle promotion and other needs.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE