Basic parameters and mechanisms of cardiovascular hemodynamics in children from disadvantaged families at relative rest in functional stress tests
Фотографии:

ˑ:
Dr.Biol., Associate Professor A.V. Nenasheva
Ph.D., Associate Professor A.S. Aminov
Institute of Sport, Tourism and Service, South Ural State University, Chelyabinsk
Keywords: allostasis, allostatic load, function tests, cardiovascular hemodynamics.
Introduction. Among the problems of developmental physiology, psychology, medicine, correctional pedagogics is social and biological rehabilitation of pupils of special educational institutions, since this category of children is eligible for full state support [3]. Present-day orphanhood as a social problem should be the subject of the interdisciplinary medical-psychological-pedagogical research and target area, putting forward the task of social rehabilitation of children, correction and compensation of abnormalities [2, 3].
Living and adaptation of the children's body to socially disadvantaged environment within the modern understanding of the problems of stress and adaptation may be considered from the perspective of the theory of allostasis, which literally stands for the achievement of stability through change [10, 11]. According to B.S. McEwen, allostasis and chronic stress are not identical. Allostasis is an alternate state of the body, developed under the influence of multiple, permanent exposure of stress factors, both undramatic and threatening well-being or even human life. Stability of the internal environment during allostasis is ensured by the attained dynamic equilibrium of homeostatic masses at a new level, which involves tension of most mechanisms of adaptation. Owing to allostasis the autonomic nervous system, the cardiovascular system, the metabolic and immune systems protect the human body, reacting to the internal and external stress. Stress adaptation is accounted for allostatic load. Allostatic load concentration falls into the category of after-effects of permanent or repeated activation of mediators of allostasis (stress hormones), ineffective functioning of the allostatic system. High stress hormone level in a week, month or year can result in the accumulation of allostatic load and cause pathophysiological changes [4-9].
The purpose of the study was to develop and estimate the efficiency of comprehensive rehabilitation measures based on the mechanisms of formation of allostasis and allostatic load in children from disadvantaged families.
Materials and methods. As of from 2010 to 2014, a total of 664 Chelyabinsk-based children aged 6-14 years were examined: from the Social Rehabilitation Center (SRC) for Minors - 327; from the Municipal Educational Institutions (MEI) № 118, 45 - 337. The children were examined at the time of entering the SRP with due regard to the adaptation period. The bioimpedance tetrapolar rheopolygraphy based on the "Kentavr II PC" computer system by "Microlux" [1] was employed to record the indicators of central and peripheral hemodynamics.
Results and discussion. Figures 1 and 2 illustrate the generalized results of deviation of the indicators of cardiovascular hemodynamics in the children from disadvantaged families compared with children from well-to-do families. Negative social environment contributes to the development of allostasis of the hemodynamic system as early as at the age of 6-10 years. The allostatic signs of the cardiac activity in 6-10-year-olds from the Social Rehabilitation Center (SRC) are: high myocardial contractility compared with children from well-to-do families, which enables to normal EF at decreased SV, Fw. High blood pressure preserves oxygen delivery - DO2i. Negative social environment contributes to the development of allostasis of the hemodynamic system as early as at the age of 6-10 years. It is expressed in relatively high blood pressure and a tendency to cardiovascular (CVS) performance deterioration, which is confirmed by Pi and Ci. The changes in the cardiovascular hemodynamics in this category of children are diversified and dependent on the type of load. In general, the hemodynamic shifts can be characterized as compensatory-adaptive, since three essential parameters remaining unchanged in all stress tests are as follows: MBV, saturation and oxygen delivery (SpO2, DO2i). It is the orthostatic test that affects most children of this age. This test is characterized by the low indices of SV and FPA, which reflects a robust blood volume regulation system in 6-10-year-olds from SRC. The cold pressure test causes the most adaptive response. The most typical reactions to stress tests are actively changing vascular tone, pulsation of APA, FPA; myocardial contractility. The direction of these changes is determined by the type of functional load.
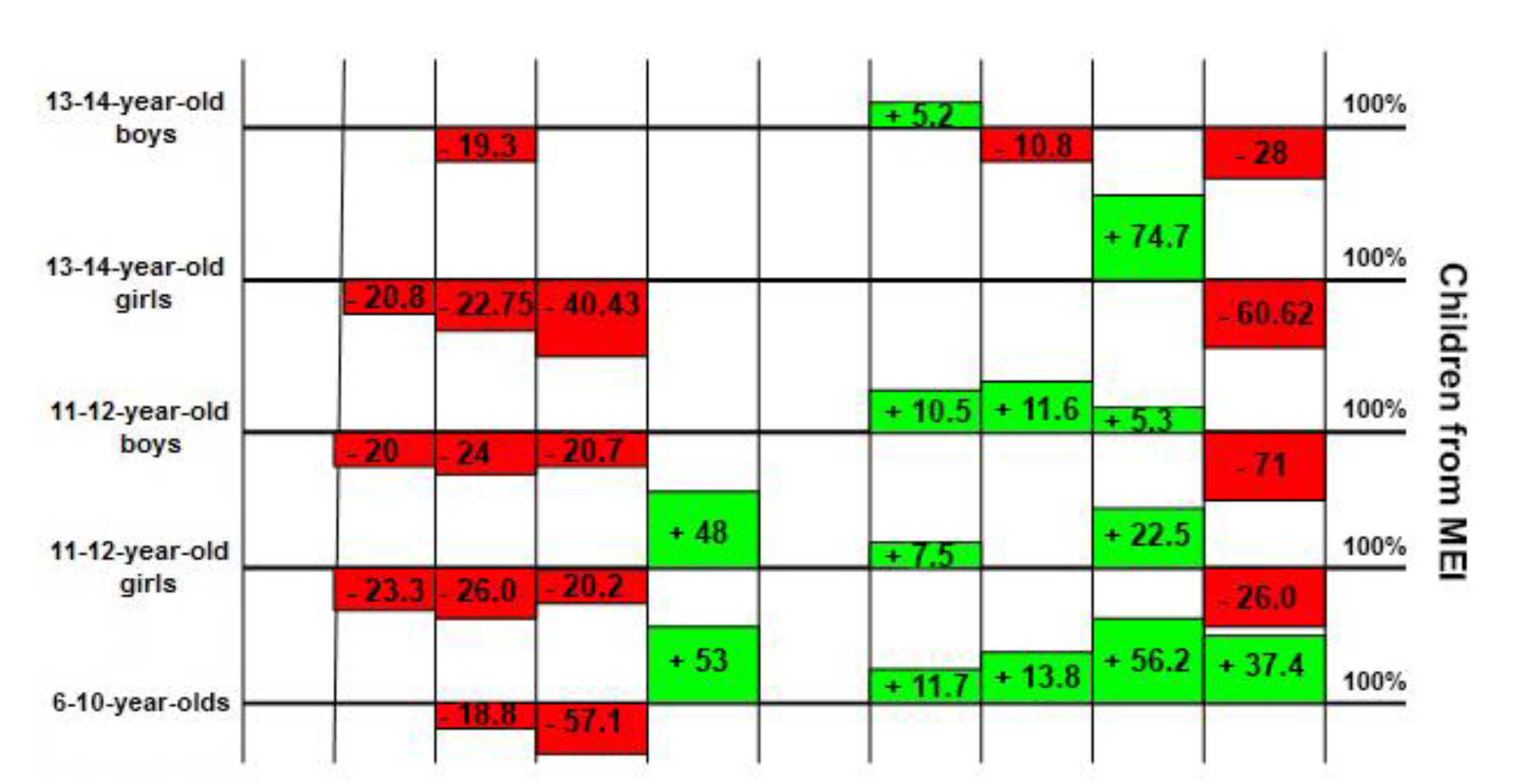
HR – heart rate, bpm; MBV – minute blood volume, l/min; SV – stroke volume, ml;. Fw – diastolic filling wave, MOhm; Нi – Hiter-index, MOhm/ms; EF – ejection fraction, %; SBP and DBP – systolic and diastolic blood pressure, mm Hg; APA – arterial pulse amplitude, MOhm; FPA – finger pulse amplitude, MOhm.
Fig. 1. Deviation of cardiovascular hemodynamic indices (%) in children from disadvantaged families
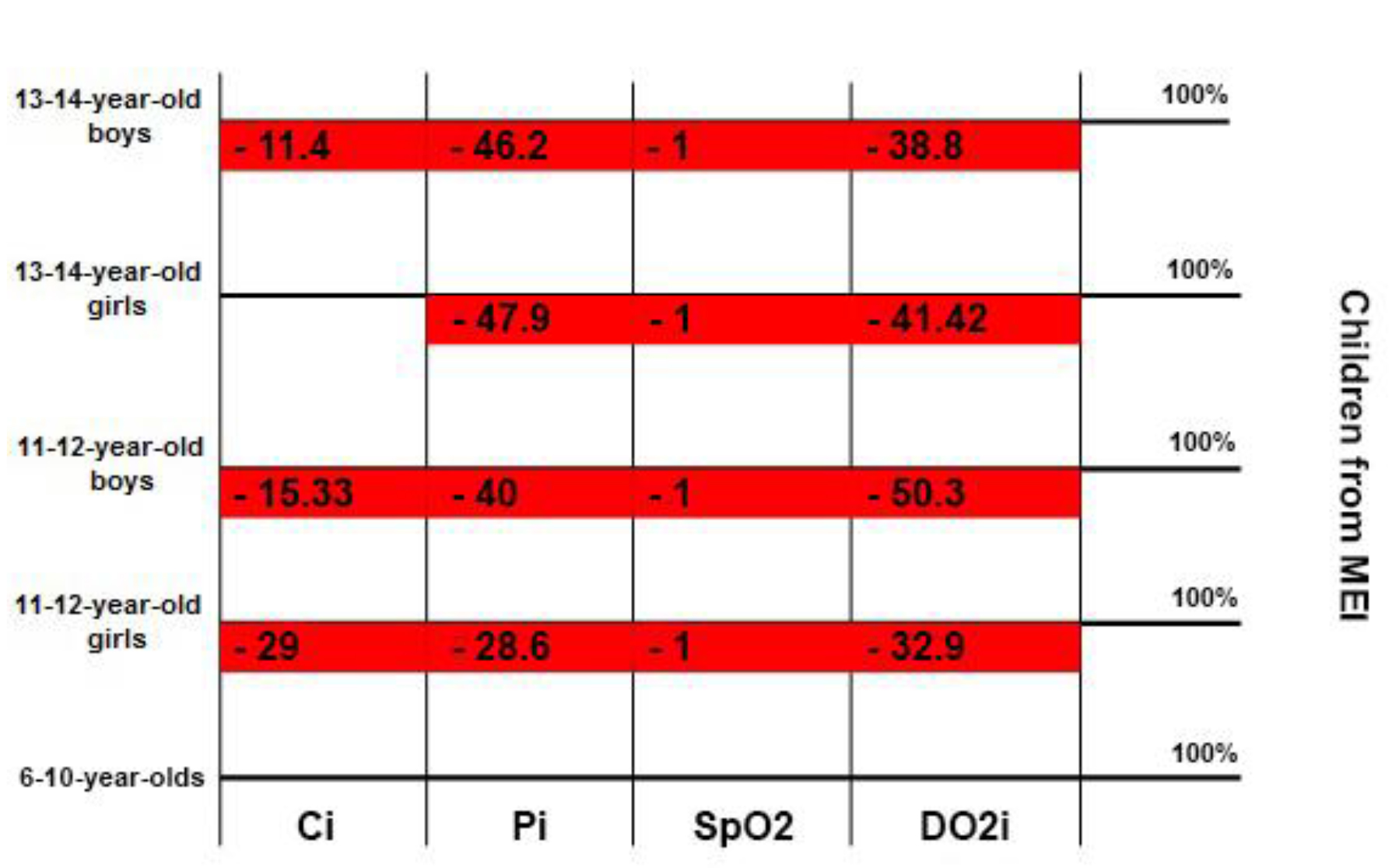
Ci – cardiac index, l/min/m2; Pi – cardiovascular system performance index, unit; SpO2 – saturation (arterial hemoglobin oxygen saturation in percent); DО2i – О2 delivery index, ml/min/m2.
Fig. 2. Deviation of integrated indices of cardiovascular hemodynamics (%) in socially neglected children
At the age of 11-12 years, the development of allostasis is still in progress in children from disadvantaged families. The effects of functional loads are mostly realized by means of changes in the cardiac performance characteristics, as opposed to girls from well-to-do families, whose adaptation is based on reactive changes occurring at the level of blood vessels. The most labile indicators in the girls from the SRC are HR and EF, the nature of APA and FPA. high SBP and DBP, HR, decreased Pi indicate allostatic load in boys from the SRC. The hemodynamic changes cannot be evaluated positively, as the DO2i values differ greatly (lower by 1.5-2) initially and under all functional loads.
The 13-14-year-old boys "at rest" were observed to have fewer intergroup differences in their cardiac activity. The differences were mostly registered at the level of vascular haemodynamic signs. All functional loads caused ambiguous and more significant hemodynamic changes at the level of blood vessels in the children from the SRC. What the children from the SRC have in common are reduced APA, SpO2 and ever-low DO2i. The most typical reaction of the boys from the SRC to functional loads is increased Pi, except for mental work load, under which this parameter decreases; increased SBP or DBP. In general, with age maladaptive reactions of the CVS to functional stress tests develop in the children from the SRC, which reflects the cumulative effect of the allostatic load. It is mental and physical load tests that cause the most pronounced maladaptive states.
Conclusion. The development of allostasis is typical for children from disadvantaged families, which is expressed in the establishment of dynamic equilibrium of the leading hemodynamic parameters at a new physiological level. Hemodynamic support of the body of children at rest and during functional loads is provided by an increase in the number of regulatory mechanisms.
References
- Aminov, A.S. Monitoring sostoyaniya zdorov'ya i fizicheskogo razvitiya podrostkov 12–15 let v razlichnykh usloviyakh prozhivaniya (Monitoring of health and physical development of teenagers aged 12-15 years in different conditions of residence) / A.S. Aminov, A.V. Nenasheva, E.V. Zadorina, E. Baymukhametova // Vestnik Yuzhno-Ural'skogo gosudarstvennogo universiteta. Seriya «Obrazovanie, zdravookhranenie, fizicheskaya kul'tura». – 2013. – V. 13. – № 4. – P. 48-53.
- Astakhov, A.A. Fiziologicheskie osnovy bioimpedansnogo monitoringa gemodinamiki v anesteziologii (s pomoshch'yu sistemy «Kentavr»): V 2 t. (Physiological basics of bioimpedance monitoring of hemodynamics in anaesthesiology (using "Kentavr" system): In 2) / A.A. Astakhov. – Chelyabinsk, 1996.
- Kuchma, V.R. Sovremennye mediko-sotsial'nye problemy detey-sirot (Current medical and social problems of orphans) / V.R. Kuchma, O.Yu. Milushkina // Gigiena i sanitariya. – 2003. – № 5. – P. 39–42.
- Carlson, E.D. Chamberlain, R.M. Allostatic load and health disparities: a theoretical orientation / E.D. Carlson // Res Nurs Health. – 2005. – V. 28, N 4. – P. 306–315.
- Clark, M.S. Environmental stress, psychological stress and allostasis load / M.S. Clark, M.L. Bond, J.R. Hecker // Psychol Health Med. – 2007. – V. 12, N 1. – P. 18–30.
- Day, T.A. Defining stress as a prelude to mapping its neurocireuitry: no help from allostasis / T.A. Day // Prog neuropsychopharmacol Biol Psychiatry. – 2005. – V. 29, N 8. – P. 1195–1200.
- Goldstein, D.S. Allostasis, homeostasis and the nature of stress / D.S. Goldstein, Mc Ewen B.S. // Stress. – 2002. – V. 5, N 1. – P. 55–58.
- Johnston-Brooks, C.H. Chronic stress and illness in children: the role of allostasis load / C.H. Johnston-Brooks, M.A. Lewis, G.W. Evans, C.K. Whalen // Psychosom Med. – 1998. – V. 60(5). – Р. 597–603.
- Korte, S.M. The Darwinian concept of stress: benefits of allostasis and costs of allostatic load and the trade-offs in health and disease / S.M. Korte, J.M. Koolhaas, J.C. Wingfield, Mc Ewen B.S. // Neurosci Biobehav Rev. – 2005. – V. 29, N 1. – P. 3–38.
- McEwen, B.S. Stress: hormonal and neural aspects / B.S. Mc Ewen, S. Lupien // in book: Encyclopedia of the human brain. Ed.-in-chief. V.S. Ramachandran. – 2002. – Academic Press. – V. 4. – P. 463–474.
- McEwen, B.S. The concept of allostasis in biology and biomedicine / B.S. Mc Ewen // Norm Behav. – 2003. – V.43, N 1. – P. 2–15.
Corresponding author: isaeva-susu@yandex.ru


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE