Rhythmic Thermal Exposures as a Non-Drug Method of Rehabilitation of Functional Status of Athletes after Strenuous Physical Load
Фотографии:

ˑ:
N.A. Fundin, professor, member-correspondent of Russian Academy of Medical Sciences
S.Ya. Klassina, Ph.D.
Research Institute of Normal Physiology named after P.K. Anokhin, Russian Academy of Medical Sciences, Moscow
Yu.E. Vagin, professor
First Moscow State Medical University named after I.M. Sechenov, Ministry of Health and Social Development of the Russian Federation, Moscow
Key words: sport, recovery, functional status of athlete, rhythmic thermal effects.
Introduction. Fast and effective recovery of an athlete after strenuous physical exercise is a determining condition of his good sports performance. Nowadays there is a variety of recovery methods, but the priority is given to non-drug methods of restoration of athlete's functional status. This is due to the fact that non-drug rehabilitation procedures are noninvasive, safe, effective and easy to use [4]. Local rhythmic thermal effects (RTE), synchronized with the rhythm of breathing and directed to skin of the nasolabial triangle of an athlete can be attributed to such rehabilitation effects. Their effectiveness was shown when restoring the functional status of persons exposed to emotional stress [2, 3].
The purpose of the study was to consider the effects of rhythmic thermal effects as a non-medicated method of restoration of the functional status of athletes after strenuous exercise.
Materials and methods. 19 males aged 18-27 (athletes and those keeping fit) were involved in the study. Each testee was examined twice, when they were to do physical exercise of increasing intensity on a cycle ergometer under medical-biological control. The interval between the first and the second examination was 7 days. During the first examination an athlete recovered after the exercise sitting on the cycle ergometer (without cycling), and during the second - also sitting on the cycle ergometer, but being subject to RTE. The recovery time in both cases was standard - 6 minutes.
RTE were carried out by means of the «Vita-Therm» device («Neurosoft», Ivanovo), the thermal element of which was fastened in the nasolabial triangle of the testee. The device helped set the temperature of the thermal stimulus which was 30оС in this survey. In this case, the heat exposure to the skin of the testee was carried out in accordance with the rhythm of his breathing, i.e. the thermal element switched on during breathing-in and off during breathing-out, so ultimately the testee could unconsciously regulate the heat supply by changing the breathing pattern.
During the examination the testee was in the following functional statuses:
- Initial state (background) - 2.5 minutes when the testees were sitting on the cycle ergometer without cycling.
- Graduated physical load where the first stage was 60W, and the subsequent stages consistently increased in increments of 10W to the moment when the testee refused to perform the work (Nmax load). It should be noted that the load test was carried out against the background of the constant speed of cycling being 7 km/h, and the duration of the load test was determined by the refusal of the testee to perform further physical work.
- Recovery - 6 minutes. In the first examination the testee stopped cycling and sat quietly on the cycle ergometer during the recovery, and in the second one he recovered on the cycle ergometer against the background of RTE.
For load testing the cycle ergometer «Sports Art 5005» was used, and the testing was conducted under the control of electrocardiography (second Nehb lead) using a computer complex «Poly-Spectrum-8» («Neurosoft»). So, it helped monitor heart rate (HR, bpm) throughout the examination, and ECG while in the initial state and during the recovery period of spectral parameters: total spectrum power (TP, mc2), power of very low frequency (VLF, mc2), low frequency (LF, mc2) and high frequency waves (HF, mc2 ), as well as a number of derived indicators (LF norm, n.u., HF norm, n.u., LF/HF, %VLF, %LF, %HF) [5]. Real pedaling speed (V, km/h) was registered using «SIGMA – bc-509” (Germany) equipment, its sensor was attached to a pedal of the cycle ergometer. In addition, in the background and during the 1st, 3rd and 6th minutes of recovery systolic (SBP, mmHg) and diastolic (DBP, mmHg) blood pressure were measured, the vegetative index of Kerdo was evaluated by calculation (VIK, % = 1- DBP/HR) [1], the testees were interviewed about their subjective general state.
The data obtained were statistically processed using the «Statistica 6.0» package. To assess the significance of differences in indicators the non-parametric Wilcoxon test was used.
Study results and discussion. Analysis of the obtained physiological parameters revealed that the use of RTE as a means of recovery of athletes after strenuous physical exercise to muscular failure had a modulatory effect on the vegetative balance, functioning of the cardiovascular system and the general state of the testees.
Figure 1 shows histograms of the mean values of systolic blood pressure (SBP, mmHg), heart rate (HR, bpm), Kerdo index (VIK, %) of the testees in the background, at the time of muscular failure and after recovery. It is clear from the figure that, the mean values of vegetative indicators at maximum load increased significantly compared to the background level, resulting in a significant increase of systolic blood pressure (SBP) from 119.8±3.5 to 150.1±5 mmHg (p<0.05), increase of heart rate (HR) from 78.6±2.6 to 151.0±3.8 bpm (p<0.05), increase of Kerdo index (VIK) from 1.3±3.7 to 48.9±2.3% (p<0.05) in the first examination (recovery without RTE). Similar dynamics of these parameters was observed in the second examination too (recovery with RTE), where SBP significantly increased from 115.7±2.9 to 134.1±3.4 mmHg (p<0.05), HR from 81.4±3.1 to 151.4±4.7 bpm (p<0.05), and VIK from 15.2±2.7 to 52.1±1.9% (p<0.05). The fact that all of the above indicators significantly increased at the time of muscular failure suggests that strenuous exercise to failure causes a sharp increase in sympathetic effects on the heart of each of the testees.
The dynamics of these parameters after the load was completely dependent on the method of recovery - with or without RTE. Thus, after recovery without RTE SBP decreased insignificantly to 119.9±2.5 mmHg, while heart rate decreased significantly and after the recovery was 102.5±3.0 bpm (p<0.05), VIK decreased significantly to 28.9±1.9% (p<0.05). After recovery against the background of RTE (with RTE) SBP decreased to 114±3.1 mmHg, heart rate and VIK decreased significantly and after recovery were 94.3±3.5 bpm and 25.8±2.9% (p<0.05) respectively. Thus, regardless of the recovery type, the dynamics of all vegetative indicators was characterized by a return to the background level.
Due to the fact that the original backgrounds of these parameters were different in the first and second examinations (Figure 1), a comparative analysis of the relative shifts of these indicators in relation to their initial background was carried out to address the issue of the effectiveness of RTE as a recovery technique. Table 1 shows the deviation values of these indicators from their background values after the recovery, in other words, the values of relative shifts of indicators (in percentage) compared to the initial background.
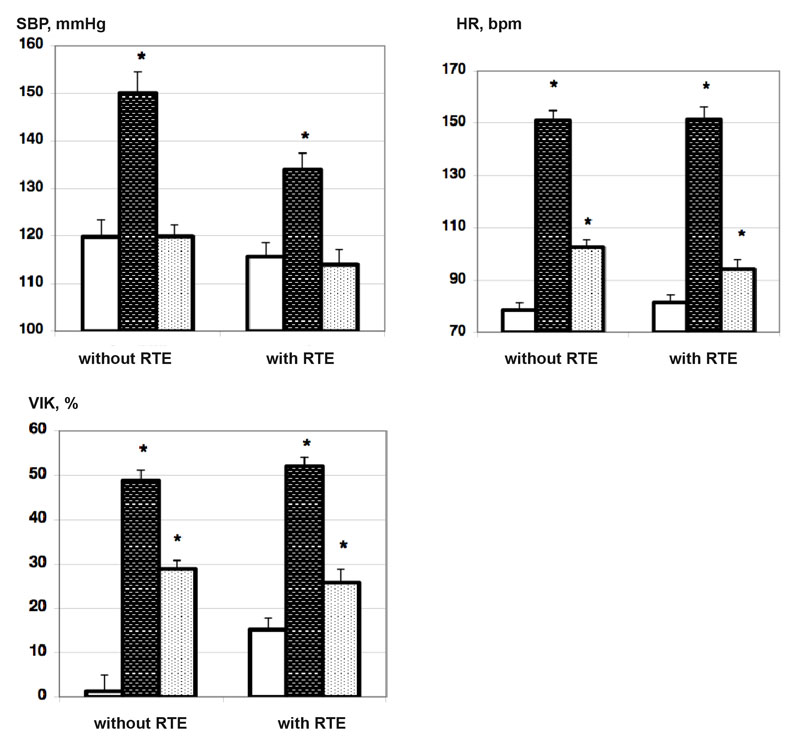
Figure 1. Histograms of mean values of systolic blood pressure (SBP, mmHg), heart rate (HR, bpm), Kerdo index (VIK, %) of the testees in the background (white bars), at the time of muscular failure (dark hatched bars) and after a 6-minute recovery (light hatched bars).
Legend: * – p<0.05 in relation to the background (non-parametric Wilcoxon test) (n=19 persons)
Table 1. Shifts in systolic blood pressure, heart rate, Kerdo index of the testees in relation to the initial background after the recovery with and without RTE (n=19 persons), M ± m
|
Indicators tested, % |
Recovery without RTE |
Recovery with RTE |
Shift differences significance |
|
SBD shift |
0.7 ± 4.2 |
-1.2 ± 2.2 |
|
|
HR shift |
35.0 ± 4.6 |
22.5 ± 2.6 |
p<0.05 |
|
VIK shift |
446.9 ± 103.9 |
286.5 ± 116.4 |
|
Note. p<0.05 in accordance with the non-parametric Wilcoxon test.
Table 1 shows that after a physical exercise to failure and a subsequent 6-minute recovery the relative shifts of vegetative parameters with respect to the initial background were different. Thus, during the recovery without RTE a small positive shift of SBP was observed along with a positive shift of HR and a significant positive shift of the VIK indicator relative to the initial background, showing the lack of recovery among the testees and the remaining quite high level of sympathetic effects on the heart. During the recovery on the background of RTE (recovery with RTE), SBP, on the contrary, had a negative shift in relation to the background, while HR and VIK indicators improved, although all of them were lower than during the recovery without RTE. Moreover, the shift of HR during the recovery on the background of RTE was significantly smaller than the one during the recovery with RTE (p<0.05). This implies that after strenuous physical exercise the recovery on the background of RTE is more effective due to a more significant weakening of sympathetic effects on the heart, decrease of SBP and HR observed.
After the recovery the testees were surveyed about how they feel after exercise. It was revealed that while after the recovery without RTE the testees complained of fatigue, after the one with RTE they, on the contrary, felt lightness (2 persons), pleasant warmth (4 persons), increased activity (5 persons), vitality (3 persons), disappearance of fatigue (1 person) and 4 persons felt muscles relaxed. All this may be evidence in favor of RTE as a recovery method that helps athletes feel better.
All these changes are probably due to the trigeminal nerve endings located in the nasolabial triangle. Rhythmic thermal effects irritate these nerve endings, so the impulse along these nerves enters vasomotor and respiratory centers in the medulla oblongata, thus determining the adjustments in the mechanisms of cardiohemodynamic indicators.
To study the effect of RTE on the shifting of vegetative balance heart rate of the testees was subject to spectral analysis in the initial state (background) and after recovery. Table 2 shows the mean values of the spectral analysis of heart rate (TP, %VLF, %LF, %HF) of the testees in the background and after recovery.
Table 2. Mean values of the spectral analysis of heart rate of the testees in the background and after recovery with and without RTE (n=19), M±m
|
Indicators |
|
Recovery without RTE |
Recovery with RTE |
Significance of differences of similar indicators after recovery, р |
|
TP, mc2 (2400-4500) |
background |
5892±768 |
6665±1486 |
|
|
After recovery |
4158±1196 |
4330±858 |
|
|
|
%VLF (15-30) |
background |
38.3±3.2 |
37.2±3.3 |
|
|
After recovery |
55.1±3.3* |
37.5±3.6 |
<0.05 |
|
|
%LF (35-40) |
background |
45.4±2.7 |
46.9±2.7 |
|
|
After recovery |
35.2±2.7* |
45.9±3.1 |
<0.05 |
|
|
%HF (15-25) |
background |
16.4±1.7 |
15.8±2.6 |
|
|
After recovery |
9.8±1.2* |
16.7±2.2 |
<0.05 |
* – p<0.05 – significance level of differences of indicators in the «background» state and «after 6 minutes of recovery» in accordance with the non-parametric Wilcoxon test. Normal ranges for each indicator are provided in parentheses.
It is obvious that during the recovery without RTE the total spectral power of heart rate (HR) tends to reduce from 5892±768 to 4158±1196 which can be regarded as its normalization. The spectral rhythm components change: %VLF significantly increases from 38.3±3.2 to 55.1±3.3% (p<0.05), %LF and %HF significantly decrease from 45.4±2.7 to 35.2±2.7% and from 16.4±1.7 to 9.8±1.2% (p<0.05) respectively. It is known that the increase of VLF-waves and decrease of HF-waves in the structure of heart rate are a clear evidence of strengthening sympathetic effects on the heart of the testees [4].
During the recovery with RTE the total spectral power of heart rate (HR) normalizes too. A slight tendency towards the %LF decrease and the %HF increase is observed against the background of stable %VLF indicator. All this suggests that RTE against the background of a decrease of the total spectral power of heart rate help maintain the initial ratio of individual components of the spectrum. However, it must be stressed that after the recovery against the RTE background the share of HF-waves was 16.7±2.2%, that being significantly higher than during the recovery without RTE – %HF=9.8±1.2% (p<0.05). Thus, while during the recovery without RTE the level of sympathetic effects on the heart does not decrease and even significantly increases (p<0.05), during the recovery with RTE, on the contrary, a shift of the vegetative balance towards weakening of sympathetic effects is observed.
Figure 2a shows the dynamics of the mean heart rate values in the background («background»), at the time of muscular failure (N max) and after the 1st (b1), 3rd (b3) and 6th (b6) minutes of recovery.
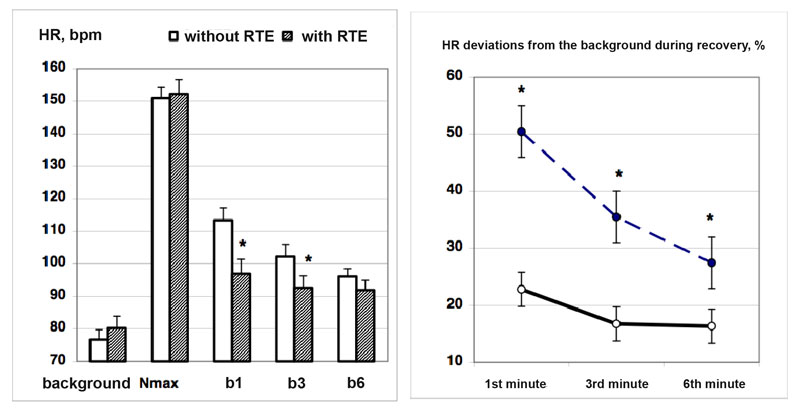
Figure 2. Mean HR values in the background («background»), at the time of muscular failure (N max) and after the 1st (b1), 3rd (b3) and 6th (b6) minutes of recovery (а), as well as relative deviations of HR from the background level in % after the 1st (b1), 3rd (b3) and 6th (b6) minutes of recovery (b).
Note. * – p<0.5 difference in indicators during the recovery without RTE (white bars and a dashed line) and with RTE (hatched bars and a solid line)
As seen from Figure 2, the recovery process is accompanied by a decrease in HR both with and without RTE. HR decreases sharply already during the 1st minute of recovery (b1), and during the recovery with RTE the HR drop is significantly more pronounced. Thus, HR at the background of RTE by the end of the 1st minute of recovery was 96.9±3.7 vs 113.4±3.8 bpm during the recovery without RTE (p<0.05). During the 2nd minute of recovery HR was 92.6±3.7 vs 102.2±2.4 bpm (p<0.05) respectively. In spite of the fact, that by the end of the 6th minute the difference in HR for these two ways of recovery was insignificant already, full recovery never happened.
Figure 2b shows relative deviations of HR from the background level (%) after the 1st (b1), 3rd (b3) and 6th (b6) minutes of recovery. It is obvious that during the recovery at the background of RTE the deviations of HR from the background level during the 1st, 3rd and 6th minutes are significantly less than during the recovery without RTE (p<0.05). Thus, the recovery of the testees at the background of RTE is faster and more effective, since the HR deviation from the background level during the 6th minute was 16±3% vs 27.4± 4.5 % (p<0.05) without RTE.
Conclusion. Strenuous physical work to failure leads to depletion of athlete's physiological capacities, therefore it is crucial to select a subsequent method to restore his functional status. Assuming that the nature of the course of the rehabilitation process can be modulated using adequately selected non-drug external exposures, the use of rhythmic thermal effects as a recovery method was proved to be highly effective. It is shown that rhythmic thermal effects on the area of nasolabial triangle, synchronized with the rhythm of breathing, can be used as a fast and effective means of restoring the functional status of an athlete after strenuous physical exercise. Rhythmic thermal effects not only contribute to the normalization of vegetative balance, lower blood pressure and HR, improvement of subjective general state of an athlete, but also accelerate the process of HR recovery over time. The use of RTE in the practice of training and competitive activities can be an effective way to enhance physical performance of athletes.
References
- Vein, A.M. Dystonia / A.M. Vein, A.D. Solov'eva, O.L. Kolosova. – Moscow, 1981. – 318 P. (In Russian)
- Glazachev, O.S. The effect of local rhythmic thermal effects of varying intensity, synchronized with the rhythm of breathing on the dynamics of human functional status / O.S. Glazachev, S.Yu. Klassina, A.A. Koryagin, N.A. Fudin // Vestnik novykh meditsinskikh tekhnologiy. – 2003. – V. X, № 4. – P. 27–38. (In Russian)
- Klassina, S.Ya. A complex of rehabilitation exposures to compensate for the effects of psychoemotional stress / S.Ya. Klassina // Fiziologiya cheloveka. - 2007. – V. 33, № 5. – P. 54– 62. (In Russian)
- Fudin, N.A. Medicobiological technologies in sport / N.A. Fudin, A.A. Khadartsev, V.A. Orlov. – Moscow, 2011. – 460 P. (In Russian)
- Task Forсe of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart Rate Variability. Standards of Measurements, Physiological Interpretation, and Clinical Use // Circulation. – 1996. – V. 87. – P. 1043.
Corresponding author: klassina@mail.ru


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE