Enhancement of Functional State of Children with Congenital Clubfoot via Physical Rehabilitation
Фотографии:

ˑ:
N. Mykhaylova1
K. Prusik2
Ka. Prusik2
I. Grygus1
1 National University of Water Management and Nature Resources Use, Rowno
2 Academy of physical education and sport, Gdansk, Poland
Key words: children, clubfoot, physical rehabilitation.
Introduction. Congenital clubfoot has a negative impact not only on the functional status of the lower extremities, but also on the whole body of a child. Because of the limitation of physical activity in children with congenital clubfoot the state of respiratory and cardiovascular systems may worsen [2,4,5,7]. Given the fact that preschool children are intensively developing in all systems, it is necessary to use the physical rehabilitation in congenital clubfoot aimed not only at correcting the pathologic position of the feet, but also on the normal development of all body systems. Physical rehabilitation in congenital clubfoot aims to stimulate, accelerate and improve the natural course of children’s physical development [1,3,6,8,9].
The aim of the research is to prove the positive effect of physical rehabilitation on the development of the respiratory and cardiovascular systems in children with congenital clubfoot.
The methods of the research. The functional state of the children was determined using the tests of timed inspiratory (Stange’s test) and expiratory capacity (Genche’s test). By means of the breath holding time test the functional state of the respiratory and cardiovascular systems was determined.
Results and discussion. The study involved 68 preschool children with congenital clubfoot: control group (n = 34), the main group (n = 34). Healthy children (n = 34) were in the control group 2. Children of the main group were engaged in physical rehabilitation by the offered programs, and children of the control group were engaged in physical rehabilitation by general programs.
To determine the functional state of the cardiovascular and respiratory systems at the beginning and end of the study the tests of timed inspiratory and expiratory capacity were conducted. This enabled to trace the impact of the conceptual system of physical rehabilitation on the changes in the functional state of children with congenital clubfoot. The children of the main group performed physical rehabilitation, which included: general developing, special exercises, exercises for mobility development and improvement of functional state of the ankle joint, physiotherapy, therapeutic massage, orthopedic products (different removable joint-immobilizers, braces), wearing antivarus shoes.
At the beginning of the study the results of the timed inspiratory capacity test did not differ significantly in all three groups of children, the indicators were only slightly higher in healthy children (control group 2):
- the lowest indicators were found as follows: breath holding for 16 s was observed in one child of the main group, 17 s – in two children of the control group 1 and 18 s in two children in the control group 2;
- the highest indicators were as follows: 26 s in one child of the main group, 26 s in two children of the control group 1 and 29 s in one child of the control group 2.
Comparing the obtained data with the averages of children of this age (24-22 s), we can see that they are only slightly different from the norm.
Whereas the children’s age at the research beginning was 4-5 years, the slightly lower results of the Stange’s test can be explained by the fact that the children of this age start learning volitional control of breathing.
At the end of the research the results of the Stange’s test in children of the control groups 1 and 2 were not significantly changed. As a result of conducted physical rehabilitation, performance indicators of the Stange’ test at the end of the research in children with congenital clubfoot of the main group improved significantly (р<0,05) (Fig. 1):
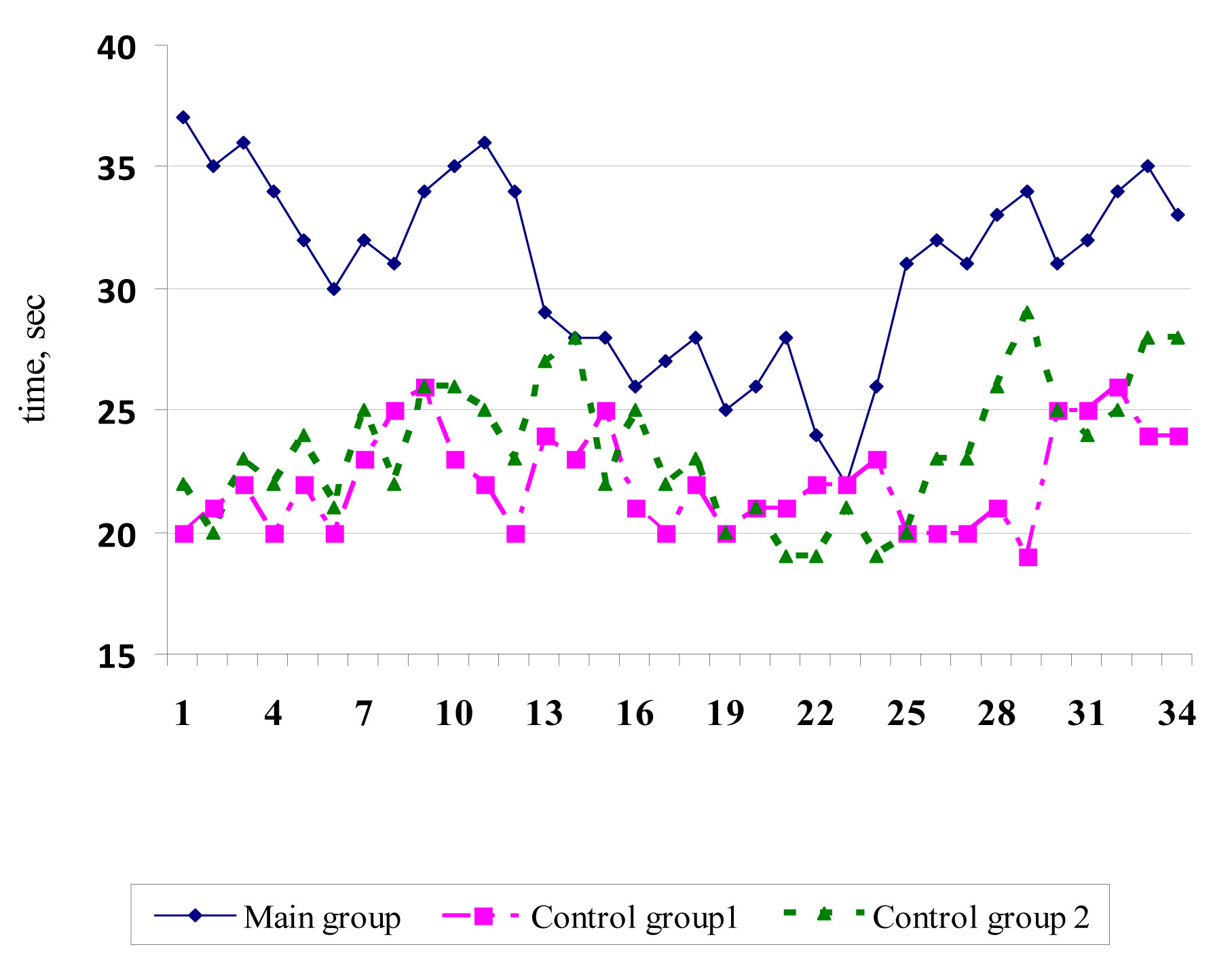
- the lowest indicators were found as follows: 25 s in one child of the main group, 19 s in one child of the control group 1 and 19 s in three children of the control group 2;
- the highest indicators were found as follows: 37 s in one child of the main group, 26 s in two children of the control group 1 and 29 s in one child of the control group 2.
Comparing the obtained data with the averages for this age (5-6 years) at the end of the research (30-22 s), we can see that they are slightly different from the norm. Along with this, significantly higher indicators in children of the main group were found.
The Genche’s functional test of timed expiratory capacity was used to analyze the lung function, this test also determines body’s resistance to hypoxia.
At the beginning of the research the results of this test performance in children of all groups did not differ significantly and were within:
- the main group: 8-13 s;
- the control group 1: 8-13 s;
- the control group 2: 8-14 s.
At the end of the research the indicators of the Genche’s test in children of the control groups 1 and 2 did not change significantly, along with this, the children of the main group had a significant increase of indicators in this test (p<0.05) (Fig. 2).
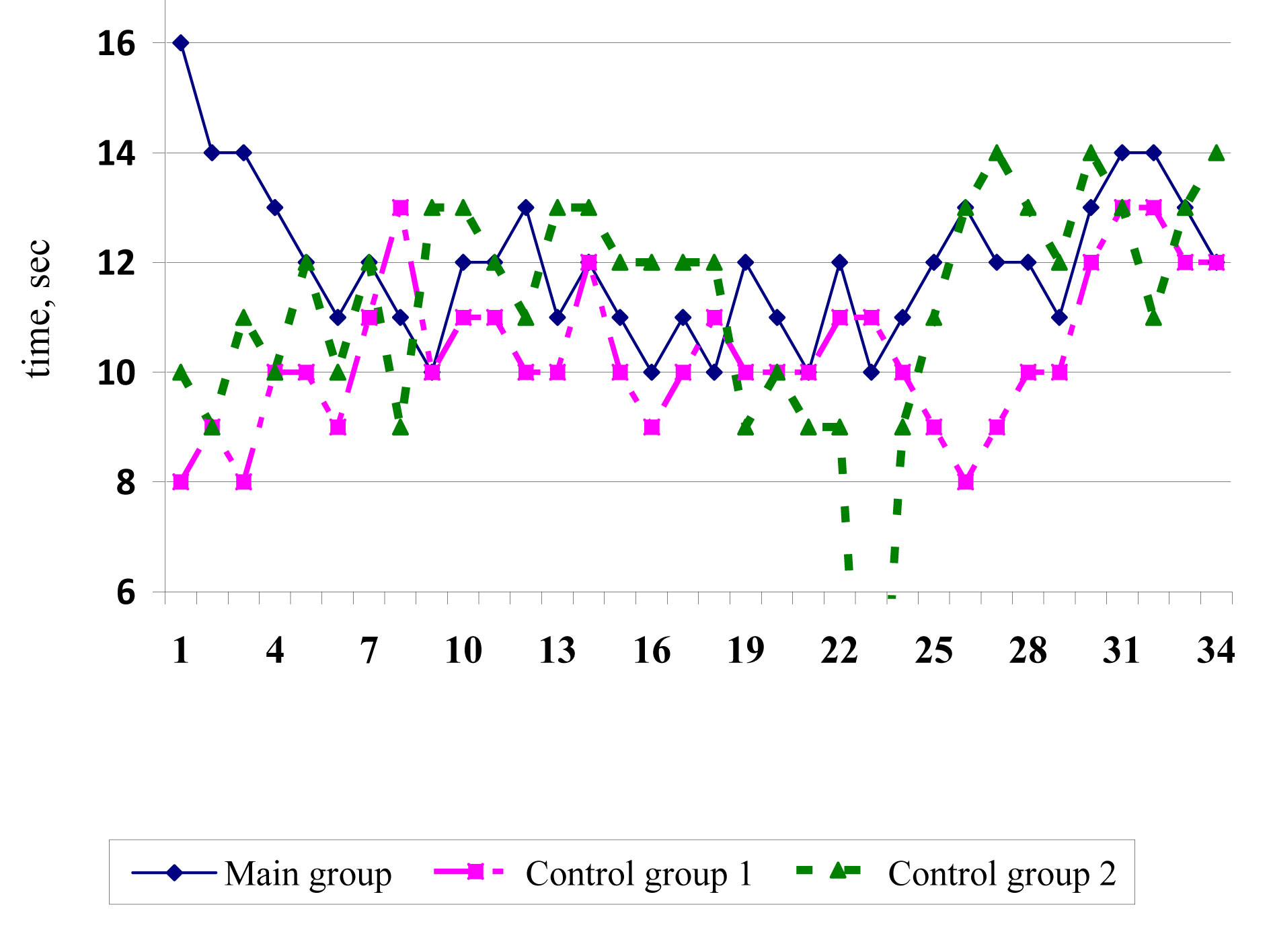
At the end of the research the performance results of this test in children were within:
- the main group: 10-16 s, at the beginning of the research they were 8-13 s;
- the control group 1: 8-13 s – the indicators have not changed;
- the control group 2: 9-14 s, at the beginning of the research they were within 8-14 s.
Table shows the average indicators of the Stange and Genche’s tests in children.
Table. Average results of the performance of Stange and Genche’s tests at the beginning and end of the research
|
Groups |
Research stages |
Stange’s test |
Genche’s test |
|
The main group |
At the beginning |
20,74±0,45 |
10,03±0,23 |
|
At the end |
30,85±0,65 *, **, *** |
11,97±0,24 *, **,*** |
|
|
The control group 1 |
At the beginning |
20,65±0,44 |
10,00±0,24 |
|
At the end |
22,12±0,34 * |
10,35±0,23 |
|
|
The control group 2 |
At the beginning |
22,65±0,45***, **** |
10,62±0,29***, **** |
|
At the end |
23,41±0,48**** |
11,44±0,28 *, **** |
Notes. * - An indicator of the reliability of differences p<0.05 between indicators at the beginning and at the end of the research within the group;
** - An indicator of the reliability of differences p<0.05 between the main group and the control group 1;
*** - An indicator of the reliability of differences p<0.05 between the main group and the control group 2;
**** - An indicator of the reliability of differences p<0.05 between the control groups 1 and 2.
Having compared the performance results of the Stange and Genche’s tests at the beginning and at the end of the research, we see a significant improvement in their results among children of the main group: Stange’s test was 20,74±0,45 s, and became 30,85±0,65 s (р<0,05); Genche’s test was 10,03±0,23 s, and became 11,97±0,24 s (р<0,05).
At the end of the research the indicators of the main group children in Stange and Genche’s tests are higher than in children of the control groups 1 and 2. The results of the children of the control group 1 were 22,12±0,34 and 10,35±0,23 s; the results of the children of the control group 2 were 23,41±0,48 and 11,44±0,28 s; the results of the children of the main group were 30,85±0,65 and 11,97±0,24 (р<0,05) s. The results confirm the positive effect of physical rehabilitation on the functional state of the cardiovascular and respiratory systems of children.
The positive trend of functional state improvement in children of the main group led to the children’s recovery.
Conclusions. The formative experiment confirmed the effectiveness of the impact of the developed concept of physical rehabilitation on the functional state of the cardiovascular and respiratory systems of the children. Significant improvements were found in terms of timed expiratory and inspiratory capacity tests in children of the main group: the Stange’s test was 20,74 ± 0,45 s, but became 30,85 ± 0,65 (p<0.05); the Genche’s test was 10,03 ± 0.23, but became 11,97 ± 0,24 (p<0.05) s. The results confirm the positive effect of physical rehabilitation on the functional state of the cardiovascular and respiratory systems of children.
References
- Vilenskaya, T.E. Physical education of primary schoolchildren / T.E. Vilenskaya. - Rostov n / D: Fenix, 2006. - P. 256 (In Russian)
- Congenital and acquired cyllosis in children and adolescents: doctors' guide / comp. by M.P. Konyukhov, I.Yu. Klychkova, Yu.A. Lapkin, L.A. Drozhzhina. – St. Petersburg, 2000. – 48 P. (In Russian)
- Bensahel, H. History of the functional method for conservative treatment of сlubfoot / H. Bensahel, B. Bienayme, P. Jehanno // J. Child. Orthop. – 2007. – Vol. 1, N 3. – P.175–176.
- Bensahel, H. Practical applications in idiopathic clubfoot: A retrospective multicentric study in EPOS / H. Bensahel, A. Catterall, A. Dimeglio // J. Pediatr. Orthop. – 1990. – Vol. 10, N 2. – P. 186–188.
- Dietz, F. The genetics of idiopathic clubfoot / F. Dietz // Clin. Orthop. – 2002. – N 401. – Р. 39–48.
- Herzenberg, J.E. Ponseti versus traditional methods of casting for idiopathic clubfoot / J.E. Herzenberg, C.Radler, N. Bor // J. Pediatr. Orthop. – 2002. – Vol. 22. – Р. 517–521.
- Noonan, K.J. Nonsurgical management of idiopathic clubfoot / K.J. Noonan, B.S. Richards // J. Am. Acad. Orthop. Surg. – 2003. – Vol. 11. – Р. 392–402.
- Pirani, S. Magnetic resonance imaging study of the congenital clubfoot treated with the Ponseti method / S. Pirani, L. Zeznik, D. Hodges // J. Pediatr. Orthop. – 2001. – Vol. 21. – Р. 719–726.
- Zwick, E.B. Comparison of Ponseti versus surgical treatment for idiopathic clubfoot: a short-term preliminary report / E.B. Zwick [et al.] // Clin. Orthop. – 2009. – Vol. 467, N 10. – Р. 2668–2676.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE