Age-Related Dynamics of Circulatory Indices of Schoolchildren (Aged 7-17) at Rest and During Exercise
Фотографии:

ˑ:
G.V. Chernova, professor, Dr.Biol.
T.E. Aleshina, Ph.D.
R.B. Taramakin
I.R. Samoylova, associate professor, Ph.D.
A.N. Romanova, Ph.D.
N.B. Litovka
Kaluga state university named after K.E. Tsiolkovsky, Kaluga
Key words: cardiovascular system, blood pressure, heart rate, schoolchildren, physical loading, orthostatic test.
Introduction. The monitoring of students' physical health improves the recreational and training effectiveness of physical education. In other words, the assessment and control of the students' functional status stimulates the introduction of new health protecting and corrective technologies in the educational practice [7].
It is known that a number of significant morpho-functional changes occur in all of child's organs and systems while he/she is growing [1, 2, 3]. The cardiovascular system (CVS) performs large functional load to protect a person's normal vital activity at all of ontogeny's stages.
Therefore, it's constantly of vital importance to track not only the age-related dynamics of the CVS indices, but also the reactions of this system in response to impact (physical load), while a change is evidenced in the functional status not only of a single system but of an organism as a whole as well and the mobilization of its adaptabilities [4].
The purpose of the study was to investigate the age-related features of cardiovascular functional indices in Kaluga schoolchildren at rest and after exercise.
Methods of study.
The study involved 602 schoolchildren (327 boys and 275 girls) aged 7-17 and enrolled in the secondary school of the town of Kaluga. They had a number of their morphological features and basic hemodynamic indicators examined, including heart rate (HR), blood pressure (BP) and HR changes with the reduction of the venus return of blood to the heart. The HR was evaluated at rest, while performing standard physical load (20 sit-ups in 30 sec) and at the recovery period (3 min), while the HR value was recorded in the prone position and right after standing up when carrying-out an active orthostatic test.
During the statistical processing of the results using modern statistical software packages, the following indicators were calculated, characterizing the overall tendency of the characteristics' occurrence as well as their variability [5]: average value, standard deviation, variation coefficient, non-sampling error and other indicators.
Results and discussion.
Blood pressure, being one of the most important indicators of peripheral hemodynamics, reflecting the functioning of the entire CVS, shows certain changes during the growth process of children (Tables 1 and 2). Thus, an increase in systolic and diastolic blood pressure (SBP and DBP respectively) is evidenced in some age-related periods.
Proceeding from the data in Table 1, boys aged 7-8 didn't show any statistically significant changes in terms of SBP, while by the age of 9 a partial reduction was observed (p<0,05), and in 11-year-olds SBP increased by 9,5 mm Hg (p<0,01). The next increase occurred by the age of 14 (p<0,05) without any further significant changes up to 17. 2 changes took place in girls as a consequence of a series of consecutive annual changes in SBP: in the age of 11 (p<0,05) and 16 (p<0,05), along with a changing tendency (p<0,1) by the age of 10 (in comparison with prior age-related periods), gender-related differences with the rise of the SBP in boys, characterized 14- (p<0,05), 15- (p<0,001) and 17-year-old children (p<0,01).
Age-related changes in DBP were evidenced mainly in boys (Table 1). A significant increase in DBP by 21,29 mm Hg (p<0,001) was observed in 9-year-olds (compared with 8-year olds) as well as a decrease by 18,02 mm Hg (p<0,001) in 10-year olds. We can also note 2 more changes: decrease (p<0,01) in 13-year-old boys in comparison with 12-year-old ones (p<0,01) and increase (p<0,001) in 14-year-old boys with no further essential changes up to the age of 17.
In the case of girls, DBP didn't undergo any statistically significant changes. Only a decreasing tendency was noted (p<0,1) in 15-year-old girls in comparison with its value in 14-year-olds. The children's gender identity stipulated for differences in the values of DBP in 7- (p<0,05), 9- (p<0,001), 15- (p<0,05) and 17-year-old children (Table 2).
It is obvious that the characteristics of the SBP and DBP dynamics should reflect the changes in pulse pressure (PP). Evidently (Tables 1, 2), the latter didn't undergo essential changes in boys and girls in a series of successive age-related periods. A significant increase of PP (p<0,001) was observed only in boys aged 11. On the other hand, in 8- and 9-year-olds (compared with prior ages) only an increasing or decreasing tendency of PP was observed. Statistically significant changes (p<0,05) were shown (in comparison with foregoing ages) in girls aged 8, 14, 16 and 17. Gender-related differences characterized 15- (p<0,001) and 17-year-old (p<0,05) children.
Table 1. Age-related changes of the circulatory indices in boys
|
Age, years |
Feature's value |
|||
|
SBP |
DBP |
PP |
CVS |
|
|
7 8 9 10 11 12 13 14 15 16 17 |
104,23±1,88 106,00±2,17 100,00±1,93* 104,44±1,95 113,94±1,95** 116,59±1,61 111,96±2,31 118,50±2,38* 116,91±1,98 116,23±2,51 113,85±1,48 |
65,65±1,76 63,21±1,80 84,50±2,05*** 66,48±1,68*** 69,03±1,71 71,88±1,48 64,46±1,69** 74,58±1,67*** 72,21±1,73 72,42±1,83 73,08±1,21 |
38,55±1,31 42,79±2,00* 38,33±1,80* 37,96±1,34 44,90±1,42*** 44,72±1,59 47,50±2,28 43,93±2,09 44,71±1,49 43,81±2,28 40,77±0,53 |
93,68±2,06 91,14±2,48 84,50±2,05* 83,56±2,04 85,42±2,25 87,25±2,73 86,71±2,89 80,70±2,03* 77,06±1,88 73,54±1,71 66,62±1,09** |
Note. In Tables 1-2 the indices are expressed in the form of average value with its non-sampling error. The varying significance among the successive age groups is shown as follows: * for p≤0,05, ** for p≤0,01, *** for p≤0,001, * for p≤0,1 (changing tendency) and the gender-related differences in brackets.
It is notable (Table 1) that the increase of SBP in boys aged 7-17 was associated with specific intervals in its changes: The 1st interval involves the ages 7 to 10, upon which no increase in SBP was noted; the 2nd period (ages 11-13) is characterized by the marked rise of its values; and the 3rd one (ages 14-17) was found with the highest indices, and whereas not only an increase in the feature's value but also a decrease in it occurred regarding the change in DBP up to the age of 13, in the case of the age of 14 it was settled at a specific level and did not change statistically up to the age of 17. Such changes of SBP and DBP did not result, in the majority of cases, in essential changes of PP.
Table 2. Age-related changes of the circulatory indices in girls
|
Age, years |
Feature's value |
|||
|
SBP |
DBP |
PP |
CVS |
|
|
7 8 9 10 11 12 13 14 15 16 17 |
102,00±1,84 106,17±2,18 101,43±3,89 109,23±2,18* 115,28±1,61* 117,95±3,06 113,28±1,89 109,57±2,54(*) 104,29±2,27(***) 112,00±2,53* 108,14±1,31(**) |
60,33±1,64(*) 61,17±1,47 66,43±3,73(***) 67,31±2,16 68,45±1,65 71,10±1,28 68,62±1,33(*) 71,90±2,20 66,79±1,71*(*) 69,00±2,00 69,30±1,02(*) |
41,67±1,30(*) 45,00±2,08* 35,00±3,45 41,92±3,33 46,83±1,44 45,70±2,83 44,66±1,72 37,67±2,76*(*) 37,50±1,22(***) 43,00±1,73* 38,84±0,66*(*) |
92,40±2,17 93,60±1,81 90,86±6,69 79,69±2,92 92,00±2,43**(*) 92,20±3,06 90,76±1,93 79,24±2,74** 69,14±1,62** 72,64±1,12* 65,77±0,91*** |
Note: For symbols' meanings refer to Table 1.
Regarding the age-related dynamics of SBP, DBP and PP of girls, it's difficult to distinguish a specific periodization, as a heterochronism of the changes manifested. This peculiarity was attributed to the heart rate (HR) too. It was observed [6] that the formation of the system of control of heart work is heterochronic in all of the age/gender-related groups of children, regardless of health groups.
Heart rate indicated the gender-related peculiarities only in 11-year old children with a higher value (p<0,05) in girls (Table 1, 2). All in all, it also showed a decrease with increasing age. As for the boys, the first decrease (p<0,05) was marked in 9-year-olds, a decreasing tendency was evidenced in 14-year-olds, while boys aged 17 had the lowest HR indices. Compared with the 7-year-olds' one, the HR value in 17-year-old boys was lower by 27,06 bpm, whereas this divergence in girls was quite close (26,63 bpm). With regard to the age-related dynamics of HR in girls, we can turn our attention to its increase in 11-year-olds (in comparison with the ones aged 10), which led to gender-related differences as well. Furthermore, starting from 14-year-olds and continuing with 15-year-olds, the HR value in those 17 years old has significantly decreased.
The values of standard deviation (σ) and variation coefficient (Cv) we calculated showed a different variation of the studied features which provided an insight into their variability level.
The described data give us an idea about the functional activity of CVS under normal life conditions of schoolchildren of various ages, although they don't give an idea of its reserve and adaptability. At the same time, it is known that the recovery process of HR after physical load is one of the most important health indicators.
The data of Figures 1 and 2 ascertain that the heart response to extra load has age-related peculiarities.

Fig. 1. Changes in the HR indices at rest and at various times after physical load in boys aged 7-17.

Fig. 2. Changes in the HR indices at rest and at various times after physical load in girls aged 7-17.
The symbols' meanings are shown in the note of Fig. 1.
When the HR in 7-10-year-olds is normalized at the end of the recovery period, the same process in senior schoolchildren is slowed down. Thus, HR in 11-year-old boys at the end of the recovery period is above normal by 19,3%, in 12-year-olds by 18,5%, in those aged 13 by 18,0%, and those aged 14 by 31,0%, at 15 by 36,8%, at 16 by 32,8% and at 17 by 51,5% respectively. As to the girls of those age-related groups, the HR got the following values: 15,0%, 4,6%, 25,1%, 33,6%, 61,6%, 41,9%, and 59,5% for 11, 12, 13, 14, 15 and 16-year olds respectively.
Thanks to the analysis 2 age-related stages can be allocated as to the reaction of the CVS to physical load. The 1st one was determined by children aged 11-13. Their pulse at the recovery period didn't exceed its index at rest by more than 25,1%. The 2nd one was related to schoolchildren aged 14-17, who showed an accelerated HR by 31,0% - 61,6%. With this in mind, it's possible to ascertain that, with increasing age, age-related unfavourable (negative) reactions of a given body to physical load may occur. A dependence of HR on body mass is expressed. The ratio of HR to body mass with increasing age significantly declines (even immediately after physical load). Thus, if in 7-year-old boys its value is 5,01 (4,44 in girls), in 17-year-olds it decreases up to 1,83 and 2,19 (in girls). In the recovery period, the data of the ratio (index) corresponded to 3,58 and 1,47 (in boys), 3,08 (in 7-year-old girls) and 1,77 in 17-year-olds. We set the indicators characterizing children aged 7-17 at rest for comparison: 3,64 and 0,98 (boys), 3,12 and 1,11 (girls). This ascertains the protractedness of the recovery period in older students. The above-described heterochronism in the dynamics of the features is clearly manifested in the values reflecting the ratios: HR/DBP, HR/PP in schoolchildren of both genders.
The assessment of the results of the active orthostatic test, characterizing the venus tone and the usefulness of the reflex mechanisms of hemodynamics' regulations [4], ascertains the satisfactory orthostatic stability (Fig. 3) in children aged 7-15. What could be considered unsatisfactory is the reaction of 16-year-old girls and 17-year-old representatives of both genders to the orthostatic test, as the increase they showed as to their HR was more than 20 bpm. What is also notable is the raising of the orthostatic test's indicators in boys aged 10 as well as the decline in 14-year-old girls in comparison with the value of increased HR in foregoing ages. Children aged 16 were the only ones who manifested gender-related differences in HR reactions.
No significant age-related dynamics with regard to the feature's occurrence was observed when assessing the orthostatic test on the basis of actual HR changes. Slight but highly significant changes in HR were noted in boys aged 9 and 17 and in girls aged 11 and 14 too. They were observed not only in the decreased, but also in the increased HR in comparison with the foregoing ages. Such changes can account for the occurrence of low orthostatic stability in children.
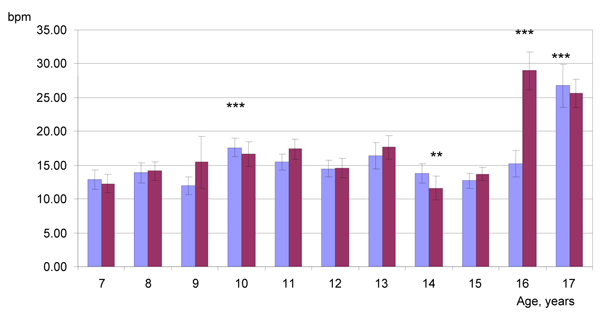
Fig. 3. Change in HR when moving from horizontal to vertical position (orthostatic test). 1st column from left to right: for boys; 2nd: for girls; along the absciss axis: time units (years); along the ordinate axis: HR indices (bmp).
Conclusion. The analysis of the findings of the studies of the CVS functional activity of 7-17-year-olds while growing revealed specific regularities in the age manifestation of the features. In most cases development of children was correlated with decrease and increase in some years of the indices showing the heterochronic manner of the CVS regulation during human ontogenesis. By the age of 17 the value of systolic blood pressure (SBP) significantly increased by 9,62 mmHg for boys and 6,14 mmHg for girls, diastolic blood pressure DBP rose by 7,43 and 8,97 mmHg correspondingly, pulse pressure (PP) did not change in boys and girls, HR dropped by 27,06 bpm (р<0,001, for boys), 26,63 bpm at р<0,001 (for girls), compared with the age of 7. The indices characterizing variability of the characteristics (σ and Cv) in age groups indicate the significant variance in SBP (Cv did not exceed 11,50±2,17%), moderate – DBP and HR (15,10±2,85%), expressed – PP (54,33±10,09%), respectively.
When using multiple approaches to identify the CVS response to additional physical load, it was proved to have age issues: while growing the unfavourable manifestations were observed in children in more cases and the rehabilitation period got longer. The exception was the orthostatic test when the unwanted effect was marked in 9, 10, 11 year olds. The allocated heterochronism in the display of the features in the aspect of CVS provokes the necessity of taking into account their peculiarities of the correct motor mode of schoolchildren.
References
- Antropova, M.V. Health problems of children and their physical development / M.V. Antropova, G.V. Borodkina, L.M. Kuznetsova et al. // Zdravookharanenie RF. – 1999. – № 5. – P. 17–20. (In Russian)
- Berezhkov, L.F. The health dynamics of schoolchildren and the value of medicobiological factors of its formation / L.F. Berezhkov, N.M. Bondarenko, A.S. Zutler et al. // Vestnik RAMN. – 1993. – № 5. – P. 8–15. (In Russian)
- Butova, O.A. The morphofunctional health evaluation of adolescents / O.A. Butova, N.A. Agadzhanyan, V.A. Baturin et al. // Fiziologiya cheloveka. – 1998. – № 3. – P. 15–18. (In Russian)
- Karpman, V.L., Belotserkovsky, Z.B., Gudkov, I.A. Test in sports medicine / V.L. Karpman, Z.B. Belotserkovsky. – Moscow: Fizkultura i sport, 1988. – 288 P. (In Russian)
- Medik, V.A. Mathematical statistics in medicine / V.A. Medik, M.S. Tokmachev. – Moscow: Finansy i statistika, 2007. – 800 P. (In Russian)
- Mukhametsinova, A.R. The functional features of cardiovascular system of junior schoolchildren from different health groups: abstract of Ph.D. thesis / A.R. Mukhametdinova. – Kazan, 2000. – 21 P. (In Russian)
- Polyakov, S.D. Monitoring and correction of physical health of schoolchildren / S.D. Polyakov, S.V. Khruschev, I.T. Korneeva. – Moscow: Airis-press, 2006. – 96 P. (In Russian)
Authors’ contacts: irus2@bk.ru, ruslan-03@ya.ru


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE