Individual academic physical education programs for special health groups for physical progress
ˑ:
D.M. Nasibullina1
T.R. Nasibullin1
PhD, Associate Professor N.A. Krasulina1
1Ufa State Petroleum Technological University, Ufa
Keywords: monitoring, correction, physical health, mental/ emotional state, express tests, individualized approach, individual training programs
Background. As reported by the university medical commissions as of 2017, more than 60% of the entrants are attributed to special health groups[3] although the academic physical education service is still not fully customizable to the needs of the students diagnosed with health disorders.The academic physical education curriculum may be effectively individualized using certain algorithms, conditional on good cooperation with and direct contributions from the students.
Objective of the study was to develop and test benefits of the academic physical education service individualizing algorithm for the special health groups.
Methods and structure of the study. The study offers the academic physical education service individualizing algorithm that may be described as the closed cyclic course including the following five modules: (1) Prior health diagnostics module to estimate the students’ physical fitness and health by detailed medical examinations – with diagnoses of health disorders, indications and contraindications for the physical education service forms, anthropometric measurements, physical fitness tests to rate physical qualities including the movement coordination; and mental/ emotional state tests; (2) Informational module that secures the learning process being supported by practical guides and theoretical materials for each student to understand own health issues and potential physical progress options; (3)Goal-setting module to formulate the individual physical education process goals with account of the health issues; (4) Practical activation moduleto offer customizable sets of physical exercises to advance one or another physical quality, with recommendations on the daily regimen, diets, ways to correct negative addictions and prevent diseases etc.; and (5) Progress test module to accumulate and analyze the individual progress test data by the prior, interim and current tests and self-tests, to fairly and timely assess benefits and drawbacks of the individual training program [5, 6].
The academic physical education service individualizing algorithm is supported by a few application software tools to put the special health groupphysical fitness tests and mental/ emotional state tests on an objective instrumental basis, including Special Health Group Information System; Physical Fitness Test System; and Individual Training Option Finding System to assist in the physical education service individualizing efforts.Benefits of the academic physical education service individualizing algorithm were tested by an experiment in 2014-17 at Ufa State Petroleum Technical University. The special healthgroup samplewassplitintoExperimentalandReferenceGroups (EG, RG, n=100 in total), withtheRGtrainedas required by thetraditional physical education service system and the EG trainings individualized with application of the academic physical education service individualizing algorithm.
The group progress was tested on a systemic basis by physical fitness, physical health and mental/ emotional state tests. The physical fitness was rated by the standing long jump, floor sitting straight bends, one-leg closed-eyes balancing, 12min walking/ running, supine trunk lift, prone push-ups andpull-ups on a horizontal bar tests. The physical health was rated by the V.I. Belov and G.L. Apanasenko express test [1, 2]. And the mental/ emotional states were rated by the standard WAM (wellbeing, activity and mood) tests. In addition, the sample was surveyed prior to and after every academic year to rate variations in the students’ attitudes to the physical education service.
Results and discussion. The post-experimental (year 3) tests showedsignificant progress of the EG versus RG in the endurance rates – viewed as the key physical quality for the overall health. More specifically, the EG and RG progress was estimated at 629.1m (24.2% growth) and 387m (16.3% growth), respectively, i.e. significantly (р<0.01) different. The pre- versus post-experimental speed-strength (standing long jump) test rates showed significant (р<0.05) progress of the EG versus RG by21.31cm (9.43%) and 11.31cm (5.26%), respectively: see Table 1 hereunder.
Table 1.EG versus RG physical health variation (pre- versus post-experimental) data
|
V.I. Belovphysical healthtest rates |
RG |
EG |
||
|
Pre-exp. |
Post-exp. |
Pre-exp. |
Post-exp. |
|
|
Headcount |
||||
|
Excellent |
0 |
0 |
0 |
2 |
|
Good |
0 |
2 |
3 |
78 |
|
Normal |
40 |
62 |
48 |
43 |
|
Poor |
60 |
36 |
48 |
17 |
|
Very poor |
4 |
4 |
5 |
0 |
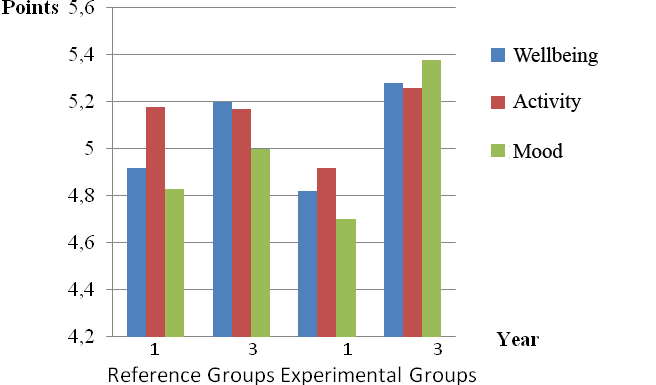
Figure 1. WAM (wellbeing, activity and mood) test rates
Conclusion. The pre- versus post experimental tests showed significantprogress of the EG versus RG in the endurance, movement coordination (static balance) and physical health test rates. The academic physical education service individualizing algorithm for special health groups was also found to significantly improve the EG mental/ emotional states, with particular benefits for the individual physical health disorders correction programs. The EG was also surveyed with the growing interest in the theoretical physical education that clearly facilitates the self-reliant physical trainings, progress and competence in the physical education matters.
References
- Apanasenko G.L. Fizicheskoezdorovyeimaksimalnayaaerobnayasposobnostindivida [Individual physical health and maximum aerobic capacity]. Teoriyaipraktikafiz. kultury, 1988, no. 4, pp. 29-31.
- Belov V.I. Entsiklopediyazdorovya: Molodost do 100 let [Health encyclopedia: Youth up to 100 years]. Moscow: Khimiya publ., 2003, 400 p.
- Valeeva E.D., Krasulina N.A., Greb A.V. Analizrezultatovmedosmotrastudentov-pervokursnikov UGNTU [Analysis of results of the medical examination of first-year USPTU students]. Aktualnyeproblemyfizicheskogovospitaniyaisporta v vuze [Actual problems of physical education and sports in higher education]. Proc. nat. scie.-method. conf., Feb 1-4 2017. Moscow: Gubkin RSOPU publ., 2017, pp. 86-89.
- Lubysheva L.I. Fizicheskayakultura i sport v vuze: innovatsionnyvektorrazvitiya [Physical education and sports in higher education: innovative vector of development]. Fizicheskayakultura, sport, turizm: nauchno-metodicheskoesoprovozhdenie [Physical education, sport, tourism: scientific and methodological support]. Proc. nat. res.-pract. conf. with intern. part. 2017, pp. 47-50.
- Nasibullina D.M., Prokhorova E.V., Mugattarova E.R. Valeologicheskayaotsenkaobrazazhiznistudentov UGNTU [Valeologichesky assessment of lifestyle of USPTU students]. Aktualnyeproblemyfizicheskogokultury, sportaiturizma [Actual problems of physical education, sports and tourism]. Proc. int. res.-pract. conf. Ufa: USTU publ., 2009, pp. 21-22.
- Nasibullina D.M., Abdullin M.G., Gimranov L.V. Fizicheskayakultura, sport izdorovye [Physical education, sport and health]. Problemyiperspektivyrazvitiyafizicheskoykultury v sovremennomobrazovanii [Problems and prospects of development of physical education in modern education]. Proc. nat. res.-pract. conf.. Ufa: Akmulla BSPU, 2010, pp. 7-10.
Corresponding author:ufa.savjulia@gmail.com
Abstract
The article analyzes one of the top priority issues of the academic physical education service – that is the service customizing for special health groups to cultivate habitual healthy lifestyles and secure physical progress of the students with health impairments. When the special health group students are exempted from physical trainings, they get into a sort of vicious circle, since the body still needs physical activity for health on the one hand, albeit suffers from physical regress due to the shortage of physical activity on the other hand. The study offers an academic physical education service individualizing algorithm that may be described as the closed cyclic course including the following five modules: (1) Prior health diagnostics module to rate the students’ physical fitness and health; (2) Informational module that secures the learning process being supported by practical guides and theoretical materials for each student to understand own health issue and the potential physical progress options; (3) goal-setting module to formulate the individual physical education process goals with account of the health issues; (4) practical activation module that offers customizable sets of physical exercises to advance one or another physical quality, with recommendations on daily regimen, diets, ways to correct negative addictions and prevent diseases; and (5) the progress test module to accumulate and analyze the individual progress test data. The academic physical education service individualizing algorithm for special health groupwas found beneficial as verified by the significant group progress in the physical fitness and health test rates, plus improvements in the mental and emotional states.


 Журнал "THEORY AND PRACTICE
Журнал "THEORY AND PRACTICE